
Ashish Shah, MD
- Assistant Professor of Surgery
- Johns Hopkins University School of Medicine
- Surgical Director, Lung Transplantation
- Johns Hopkins Cardiac Surgery
- Baltimore, Maryland
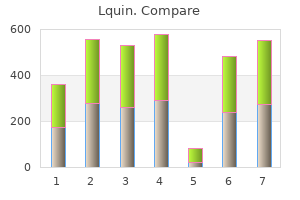
There are several laboratory studies utilized in the diagnosis and assessment of congestive heart failure in the pediatric patient antibiotic for uti cheap lquin express. A chest x-ray is one of the more useful studies in the initial assessment of a patient with suspected heart failure antibiotics japanese order generic lquin from india. This allows evaluation of heart size and contour antibiotics listed by strength lquin 500 mg generic, pulmonary vascularity antibiotic resistant bacteria generic lquin 500 mg online, presence of pleural effusions, abdominal and cardiac situs. An electrocardiogram is most useful in instances where heart failure is secondary to an arrhythmia, anomalous coronary artery, or myocarditis. Echocardiography is useful in all patients with heart failure to assess for structural anomalies, cardiac function, and cardiac chamber sizes. Other useful laboratory studies may include an arterial blood gas (in very ill patients), serum electrolytes (including calcium and magnesium levels), and a complete blood count (to help rule out the presence of anemia). Pediatric patients with heart failure will often have a mild hyponatremia, resulting from increased renal water retention rather than a true negative sodium balance. The major goals in the treatment of congestive heart failure include relief of pulmonary and systemic venous congestion, improvement of myocardial performance, and reversal of the underlying disease process (if possible). Historically, digoxin has been one of the most widely used pharmacologic agents in the treatment of heart failure in infants and children. In addition to its positive inotropic effect, digoxin exerts beneficial effects via sympathetic-inhibiting actions via baroreceptor, central, and adrenergically mediated mechanisms. Other inotropic agents used in the treatment of acute heart failure include dopamine, dobutamine, and phosphodiesterase inhibitors (milrinone and amrinone). Diuretic therapy plays an integral part in the treatment of pediatric patients with congestive heart failure. The three most commonly utilized classes of diuretics include the loop diuretics (furosemide-Lasix, bumetanide-Bumex), potassium sparing diuretics (spironolactone), and thiazide diuretics (hydrochlorothiazide). The benefits of diuretic therapy include improvement in systemic, pulmonary, and venous congestion. Spironolactone may exert additional beneficial effects by attenuating the development of aldosterone induced myocardial fibrosis, and catecholamine release. Potential complications of diuretic therapy include volume contraction, electrolyte abnormalities (hyponatremia, hypo or hyperkalemia, hypochloremia), and metabolic alkalosis or acidosis. Electrolyte balance should be carefully monitored, especially during aggressive diuresis, as the failing myocardium is more sensitive to arrhythmias induced by electrolyte dyscrasias. The use of afterload reduction is one of the newer concepts in the management of heart failure. Relaxation of arteriolar smooth muscle helps to decrease the systemic vascular resistance and augment cardiac output. Venodilatation exerts its effect on preload by increasing venous capacitance, thus lowering filling pressures. They are thought to have beneficial hemodynamic effects in patients with decreased systemic ventricular contractility, and those patients with large left to right shunts. The phosphodiesterase inhibitor milrinone is often used in the intensive care setting of acute, new onset systemic ventricle dysfunction. Treatment of chronic heart failure with the use of beta-blockers, such as carvedilol, is now an accepted practice in the adult population. The beneficial effects are thought to be derived Page 271 from the reversal of myocardial dysfunction occurring secondary to sympathetic activation and down-regulation of beta-adrenergic receptors, coronary artery vasodilatation, and possible anti-oxidant effects. The present state of knowledge for use in the pediatric population is based on anecdotal experience from unblinded, non-randomized studies of small sample size. Therefore, beta-blockers should be used with caution in infants and children with chronic heart failure until more experience is gained with these agents. Other non-pharmacologic therapeutic measures that may be considered in patients with congestive heart failure include elevation of the head and shoulders to 30 to 45 degrees, bedrest, dietary changes (higher caloric intake, and a low sodium diet in older children and adolescents), packed red blood cell transfusion, iron supplementation, and the administration of supplemental oxygen. It must be remembered that oxygen is a pulmonary vasodilator, therefore in patients with known large left to right shunt lesions, administration of oxygen will decrease pulmonary vascular resistance, increase the degree of left to right shunting, and worsen the degree of pulmonary edema. For acute pulmonary edema, several treatment methods are used which help to understand the underlying pathophysiology. Within the alveolus, the major force which holds water in the interstitial and vascular space is the plasma oncotic pressure. The force attempting to push water out into the alveolar space is the hydrostatic fluid pressure. Pulmonary edema basically occurs when the hydrostatic force pushing the fluid out, exceeds the oncotic force holding the fluid in. It is slightly positive (pushing the fluid out of the alveolus into the interstitium) when we exhale, since we exhale against partial resistance. The air pressure is negative when we inhale (which favors drawing fluid into the alveolus). To treat acute pulmonary edema, the hydrostatic force pushing the fluid out into the alveolar space can be reduced by reducing back pressure (preload and afterload reduction) by the following therapeutic measures: 1) diuresis, 2) vasodilation (increases vascular capacitance), and 3) augmenting contractility (reduces back pressure). This literally pushes the fluid out of the alveolus back into the interstitium and vascular space. With a ventilator, inspiration is under positive pressure driving the fluid out of the alveolar space. However, during exhalation, the positive pressure declines permitting the fluid to return. Other measures of historical interest only, include phlebotomy (to balance the humors) and rotating tourniquets. In patients with heart failure, the treatment plan should ultimately deal with the underlying condition. This may include surgical repair of a shunt lesion or valvular anomaly, interventional cardiac procedures, radiofrequency ablation, control of hypertension, anti inflammatory treatment for rheumatic carditis, pacemaker implantation, carnitine supplementation, adenoidectomy and weight loss for patients with airway obstruction, pulmonary hypertension and right heart failure, or cardiac transplantation. The prognosis of the pediatric patient with heart failure depends largely on the primary condition. The majority of patients with myocarditis, who present in heart failure, will improve with medical management. Patients with cardiomyopathies or hypoplastic left heart syndrome will occasionally require a heart transplant as a last resort. Those patients with arrhythmia induced heart failure will often respond well to anti-arrhythmic therapy and/or electrophysiology study and radiofrequency ablation. What is the most common congenital heart defect with a left to right shunt causing congestive heart failure in the pediatric age group True/False: Jugular venous distention is a common finding in infants with heart failure. What is the most likely age an infant with a large ventricular septal defect will begin manifesting symptoms of congestive heart failure Administration of supplemental oxygen to a child with a large left to right shunt lesion will help improve the degree of congestive heart failure. What is the dominant mechanism with which infants and young children increase their cardiac output True/False: All neurohormonal and sympathetic responses of the body to heart failure are beneficial. In the course of the interview, his mother mentions that he seems to get short of breath with exercise recently. It is especially noticeable during his swimming lessons when he tires before the other children do in his class. He has otherwise been in good health since his last physical exam in the previous year. His records for the past year show 3 office visits for minor upper respiratory illnesses, and no emergency room visits. Heart: No palpable thrill, normal 1st and 2nd heart sounds; no clicks or rubs; grade 1/6 ejection systolic murmur heard along the left sternal border with radiation to the back between the scapulae; no diastolic murmur. Extremities: Femoral pulses are slightly diminished to palpation; no peripheral edema, clubbing or cyanosis of the nail beds. An echocardiogram is performed the following day and demonstrates a coarctation of the aorta, and bicuspid aortic valve. With the advent of fetal echocardiography, these lesions are sometimes detected before birth. A list of the acyanotic lesions can be made by enumerating the structures encountered by the flow of blood through the different parts of the heart beginning with the venous side. Acyanotic congenital lesions account for 70% of all congenital heart disease, the most common of which, as isolated lesions, are ventricular septal defects (most common), patent ductus arteriosus, atrial septal defect and pulmonic stenosis.
Du Bois sorrowfully describes passing a severed black nger displayed for the public while he was on his way to work in Atlanta antibiotics cause fever purchase lquin 750 mg mastercard, we have to conclude that antibiotics and yogurt order lquin 500 mg with mastercard, like the German population during the Nazi regime infection meaning lquin 500 mg free shipping, white working-class people in the South and elsewhere largely knew about the atrocities and largely approved of them virus list discount lquin 750 mg online. Shortly before he died, I discovered that my own grandfather had participated in Klan violence in his youth. He was a semiliterate working-class Irish American who lived poor and died poor, sneered at by the rich folks he worked for; but I also believe that his sense of white superiority must have helped to produce the self con dence it took for him to go back to school as an adult and learn to read, write, and do enough arithmetic to improve his job skills. Therefore, although I believe, like Ignatiev and Garvey, that an argument can be constructed that it is actually not in poor whitesoverall economic interest to maintain racism (certainly, taking more than one generation into account), I think these authors sidestep the issue of moral culpability and its relation to social identity. Racism appears to be deeply sedimented into white psyches in a process that is newly reenforced each day. In regard to clearly identi ed racist acts of commission that require conscious intent, Ignatiev may be right. And this dependence may often operate precisely because they are themselves oppressed; that is, because their immigrant relations were a humble lot without other cultural resources from which to draw a sense of entitlement. White supremacy may be all that poor whites have to hold onto to maintain a sense of the the Whiteness Question 217 most basic entitlement to human rights, such as the right of political enfran chisement. The very genealogy of whiteness was entwined from the beginning with a racial hierarchy, which can be found in every major cultural narrative from Christopher Columbus to manifest destiny to the space race and the computer revolution. So here is the predicament: we must tell the full story of white racism in all its complexity, and this complexity cannot be fully resolved through a class analysis that sequesters the guilty as only among the rich. Yet facing the reality of whitesmoral culpability threatens their very ability to be moral today, because it threatens their ability to imagine themselves as having a socially coherent relation to a past toward which anyone could feel a positive attachment. Paradoxically, although its contributors criticize all variants of multiculturalism because, among other reasons, it tends to talk about oppression without naming any oppressors, Race Traitor is very optimistic about white cross over. Yet they interpret the increase in white crossover as signaling the fracturing of white supremacy. This position has elicited skepticism from some readers of color, whose cri tiques the journal has printed. Salim Washington and Paul Garon both have expressed concern that examples of race traitors are being romanticized. Merely to appreciate and acknowledge black in uences in dominant culture does nothing to remedy this. Garon similarly stresses that the usual economic effects of crossover are that white performers are enriched and black performers have even less chance to make a living. Garon also challenges the view (not necessarily held by Rubio) that no essential musical integrity is lost when white performers play the blues. When does the transcendence of cultural chauvinism merge into cultural appropriation Especially in a consumer society, the core of white privilege is the ability to consume anything, anyone, anywhere. The desire to cross over is itself coterminous with a colonizing desire of appropriation, even to the trappings of social identity through a hip hop clothing style. This does not mean that the culture industry transcends the racial hierarchies of existing political economies; hybridity in cultural forms does not entail a corresponding 218 Racialized Identities and Racist Subjects distribution of economic success. However, in trying to overcome unfair distri butions of nancial resources or access to cultural production, it is unrealistic to propose a voluntary self-segregation or, for example, that whites stick to white music. This means that cultural hybridiza tion is not a sufficient cause or even a necessary indicator of antiracism. We also perceive our being-for-others, or the value and meaning we have in the eyes of the Other. As Lewis Gordon argued in his interesting book Bad Faith and Antiblack Racism, white racism is generally predicated on the need and desire of whites to de ect the look of the black Other, a look that will reveal guilt, accusation, and moral de ciency (1995, esp. Sartre, who was famously pessimistic about the egalitarian potential of human relations, presented two options as to actions that can be taken toward the Other. This is the paradox of love: we want the Other to love us in a way that is absolute, unchanging, and reliable, but we want this love to be freely given without coercion. White attempts to appropriate black culture may fall into this category, as a strategy that does not seek to de ect the black look or repress it into blank sub mission but instead seeks to incorporate the black look within oneself. Such an analysis does not require a wholesale rejection of crossover, but counsels a careful scrutiny of crossover postures that would seek to erase difference. An example of such a posture would be one that Garon criticizes, the view that the blues are a transracial, universally accessible cultural form. It may be that the denial of the black speci city of blues, with the argument that suffering is available across race, is motivated by unease about what expressions of black suffering es pecially signify for white listeners. Universal suffering is nonaccusatory; black suffering is implicitly accusatory, just by making reference to black history. Thus, to incorporate the blues as a cultural form that is proper to American experience without a racial speci city helpfully de ects the potential meaning for whites of a the Whiteness Question 219 blues identi ed as black. This does not entail that white antiracists should never sing the blues, or that they cannot develop new forms of the blues, but that the blackness of the blues, or at least of its cultural genesis, should not be dismissed as irrelevant. The nal white antiracist example I will discuss is more consciously situated in a particular context and aimed at transforming white self-understanding. Katz similarly argues that the rst task of antiracism is for whites to come to understand that they are white. But where I grew up, whiteness was a substantive racial identity whose political privileges were well known and mostly considered justi ed. The cultural substance of whiteness consisted in such elements as putting peanuts in your R. Because southern whiteness has had a high degree of racial self-consciousness, then, it should be an instructive location at which to observe attempts at antiracist transformation. About fteen years ago, the University of Mississippi decided to go proactive against racism, as well as sexism, by instituting a mandatory course for all fresh men. Harrington, chair of the philosophy department, was asked to design a suitable course. Harrington established a course, university studies 101, taught it himself for a number of years, and developed a textbook that continues to be used.
Quality 250 mg lquin. Yarn Lea strength tester.
It may be preferable to assess capillary refill centrally (over the chest or forehead) and peripherally (fingers) antibiotic resistance nice discount lquin 250 mg without prescription, so that the two can be compared bacteria mod 1710 buy discount lquin 500 mg on line. Delays of 2 to 3 seconds may indicate moderate dehydration commonly used antibiotics for sinus infection cheap 500 mg lquin with visa, and more than 3 seconds in delay may indicate severe dehydration antibiotic resistance solutions buy lquin canada. Most children with clinically significant dehydration, will have 2 of the following 4 clinical findings: 1) capillary refill greater than 2 seconds, 2) tacky mucous membranes, 3) no tears, and 4) ill appearance (8). Page 341 Management the decision to hospitalize or to attempt outpatient management will be based on the clinical findings, combined with a history of fluid intake, the frequency of urination, assessment of concurrent stool losses and the response to therapy. Once a child is presumed to be dehydrated, the degree of dehydration needs to be determined. Acute weight loss can be used to determine the degree of dehydration, but accurate baseline weights in growing children are almost never known. Children with mild to moderate dehydration can be initially treated with oral rehydration. The degree of dehydration and the presence of ongoing losses dictate the volume of fluids to be administered. In either case, an additional 10 cc/kg should be given for each diarrheal stool seen. Examples of maintenance oral solutions are: Pedialyte and Infalyte, containing 45-50 mEq/L Na, 2-2. Patients with mild dehydration can potentially be managed without laboratory analysis. However, in moderate or severe dehydration, laboratory studies should be obtained to look for electrolyte abnormalities of to measure the degree of metabolic acidosis. Usually, half of the replacement therapy in addition to the maintenance fluid requirement is given over the first 8 hours, and the second half is given over the next 16 hours. However, patients with hypernatremic dehydration (serum sodium >150mEq/L) require special intervention. This is done because rapid correction of hypernatremia can result in acute brain swelling, brain herniation, and death. Therefore, care should be taken to avoid dropping the serum sodium by more than 15mEq/L per 24 hours. Once a child is adequately rehydrated, the question of when to start feedings arises. It was previously perceived that a period of "gut rest" should follow rehydration of patients with acute gastroenteritis. Numerous trials have shown that early feeding of age appropriate foods results in faster recovery. Following rehydration, children with mild diarrhea who drink milk or formula can tolerate full strength feedings. Controlled clinical trials have shown that starches, complex carbohydrates (rice, wheat, bread, potatoes, cereals), soups, fresh fruits and vegetables, yogurt, and lean meats are better choices, and well tolerated (9). Fatty foods, juices, teas, sweetened cereals, soft drinks, are poor choices, and should be avoided. Most pediatricians and experts recommend against using anti-diarrheal agents such as Imodium (loperamide), Pepto-Bismol (bismuth subsalicylate), and Kaopectate. This is more of a precaution since many studies do show some beneficial effects from these medications in patients with mild diarrhea. However, patients with mild diarrhea will get better on their own so these medications are usually not necessary. For young children with severe gastroenteritis, there is insufficient data to confirm the benefit and safety of these medications, which is why they cannot be recommended routinely at this time. What is the most common viral cause of acute gastroenteritis, and what are its associated symptoms Chapter 52-Approach to patients with gastrointestinal tract infections and food poisoning. The diagnosis can be made by antigen detection, identifying cysts in the stool, endoscopy or examination of jejunal contents. Sunken fontanelle, absence of tears, sunken eyes, sticky/tacky oral mucosa, delayed capillary refill, reduced skin turgor, inactivity/lethargy, tachycardia, hypotension. With oral rehydration, small frequent volumes 5-20cc every 5-10 minutes, advanced slowly. Her parents report that 2 weeks ago, she began to have yellowing of her eyes with subsequent yellowing of her skin when she was diagnosed with physiologic jaundice. After persistent jaundice for 5 days, her parents changed her from breast-feeding to a commercial formula. Since the jaundice appears to be worsening, her parents decided to bring her in for re-evaluation. She was born by spontaneous vaginal delivery to a G2P1 A+ mother at 39 weeks with Apgar scores of 9 and 9 and 1 and 5 minutes. She is awake, alert, in no acute distress and is easily comforted by her mother during the exam. Her skin is jaundiced, most notably in the cephalic and truncal areas, with scleral icterus. Laboratory examinations reveal a total bilirubin of 15 mg/dL, direct bilirubin of 12. She is then scheduled for a laparotomy with intraoperative cholangiogram, wedge liver biopsy and possible Kasai procedure. However, it is now known that the intrahepatic bile ducts are also affected by the disease process (1,2). The fetal type occurs in 15-35% of cases and is characterized by an earlier onset of cholestasis (1). There is an association between the fetal type and other congenital anomalies such as situs inversus, polysplenia, cardiac malformations, and other manifestations (1,2). As the names imply, the initiating event of the two types are theorized to occur at different times in development with probably very different etiologies. Research has focused on the possible etiology of the perinatal form with causes including viral infections, auto immune disease, and immune mediated damage (1,4). While there are possible candidates for the defective gene there has been no definitive identification. The signs and symptoms of biliary atresia will be dependent upon the time of presentation. Jaundice can be present at birth or it can present as late as 3 to 5 weeks of life. Other than jaundice, another common complaint is acholic stools, which are highly suggestive of cholestasis. There can be some pigment in the stool due to sloughing of cells that contain pigments. However, this pigment is only present superficially with the core of the stool remaining pale (3). Since the bile pigments are no longer released into the stool, they will be deposited in the urine leading to darker urine. On physical exam the patient will usually have an enlarged firm liver (normal averaging 4. The presence of splenomegaly is variable and more common with later presentations as part of the constellation of portal Page 343 hypertension. Later presentations are associated with the progression of the disease to biliary cirrhosis and the development of portal hypertension with failure to thrive (2). The clinical picture at this point will be dominated with findings suggestive of cirrhosis and portal hypertension such as jaundice, hepatosplenomegaly, a nodular liver, varices, ascites, and hepatic vascular bruits (1,3). Laboratory examination will show an elevated total bilirubin with an increased direct (conjugated) portion. Alkaline phosphatase will be highly elevated reaching levels higher then 5 times normal (2). There are many conditions that can cause cholestasis in the neonate and lead to jaundice. These include hepatitis (viral and other causes), sepsis, endocrinopathies, metabolic derangements, and nutritional hepatotoxicities (6). There have been diseases that are now described that were once under the heading of idiopathic neonatal hepatitis such as alpha-1-antitrypsin deficiency.
In the 3D group antibiotics used for diverticulitis lquin 250 mg, there was a higher percentage of patients with mammographically heterogeneous or extremely dense breasts (p<0 antimicrobial vs antibiotics generic lquin 750 mg fast delivery. There was a similar distribution of mammographic findings antibiotic resistance and meat order lquin 250 mg free shipping, such as presence of a mass and calcifications (p=0 antibiotics for dogs for uti purchase lquin online now. Most patients underwent radioactive seed-guided localization than wire localizations for non-palpable lesions in both groups (p<0. Fifty-nine percent of patients in the 3D group had additional imaging directed cavity margins excised based on surgeonsinterpretation vs. Thirty-eight patients (12%) in the 2D group had positive margins in main tumor specimen vs. On multivariable analysis, the use of 3D tomosynthesis compared to 2D imaging (Odds ratio=0. Conclusions: Although both hospitals had significantly different patient populations, the re-excision rates after breast conservation are relatively low. Even after accounting for these differences, 3D tomosynthesis is independently associated with a lower re-excision rate (over 50% reduction). This technique can allow the surgeon to make a better assessment of margins to direct margin excision at the index operation. This translates into decreased return to the operating room, decreased anxiety levels, and lower costs for our patients. Patients with in situ disease, neoadjuvant therapy, or prior ipsilateral breast irradiation were excluded. Data regarding re excision rate, intraoperative/final histopathologic margin width, closest margin laterality, final margin positivity, change in margin status, localization method, specimen weight, histologic subtype/grade, tumor size, and nodal status were collected. Positive margins are associated with a two-fold increase in risk of ipsilateral breast tumor recurrence. Routine circumferential cavity shave margins have been reported to half the re-excision rate. The objective of this study was to determine if selective margin resection guided by intraoperative imaging during lumpectomy can result in low margin re-excision rates. Methods: Patients with invasive breast cancer treated with breast conservation therapy from November 2011 through May 2018 were identified using an institutional surgery database and retrospectively reviewed. Patient demographics, tumor characteristics, operative details, pathology results, complications, and survival were collected. Lumpectomy specimens were labeled using radiopaque markers on 6 sides and imaged with 2 view radiograph and/or ultrasound. Additional margins were resected at the discretion of the surgeon based on the imaging. Results: A total of 175 female patients were included, and the median age was 56 years. Selective margins were resected in 102 (58%) patients, and the mean number of margins resected was 1. Twenty-seven (15%) patients had a positive margin on the lumpectomy specimen, and in 9 of those, the corresponding margin was selectively resected concurrently with only 1 persistently positive margin. The rates of seroma and surgical site infection did not different between patients who did and did not have selective margins resected. Conclusions: Using imaging-guided selective margin resection, the rate of re-operation for margin re excision was low at 11. Selective margin resection did not significantly increase the total volume of tissue excised or the risk of seroma or surgical site infection. The re-excision rate was potentially reduced by half and is comparable to that reported for cavity shave margins. We reviewed our outcomes using the device in respect to rates of positive lumpectomy margins and volumes of lumpectomy specimens. Methods: We prospectively collected the data on our first consecutive 111 lumpectomies performed during the first 12 months of use of the device from April 2015 to March 2016. This was compared to a historical cohort of 87 consecutive lumpectomies performed during the 12 months just prior to this time period. We also observed a steady decrease in lumpectomy volume as experience was gained using the device (Figure). Conclusions: these results were able to demonstrate favorable outcomes with the MarginProbe device for reducing positive margins while simultaneously reducing the size of the main lumpectomy specimen. Most centers using the device report a reduction in positive margins by about 50%. This study was unique in that it included the assessment of the lumpectomy volumes as well. Further studies with randomization to the use of this device versus other intraoperative methods of margin assessment would be valuable. A retrospective chart review of these patients was performed to determine margin status and re-excision rates during the 2 years before and 2 years after the guidelines were published in order to determine the effect on our re-excision rates. Twenty-four patients had positive margins, and 22 underwent re-excision, including 3 mastectomies. The remaining 79 patients had close margins, and 45 (57%) of these patients underwent re-excision, including 1 mastectomy. Nineteen patients had positive margins, and 17 underwent re-excision, including 2 mastectomies. Our overall re-excision rate decreased slightly; but, of the patients who had close margins, a larger proportion underwent re-excision after the guidelines were published. The guideline publication appears to have affected our institutional practices slightly, but not dramatically, as many of our surgeonspractices were comparable to the guideline recommendations prior to 2016. We continue to use clinical judgement based on patient and tumor characteristics in deciding which patients will benefit from margin re-excision. We sought to determine if utilizing MarginProbe Radiofrequency Spectroscopy could further reduce positive margin and subsequent re-excision rate, without increasing excised tissue volume, in the No Ink on Tumor era. Methods: We present a retrospective, observational review of 243 consecutive patients treated from January 2016 April 2018. All patients were treated post-adoption of Consensus Invasive Guideline of No Ink on Tumor and represent the 157 consecutive patients directly before, and 86 consecutive patients directly after, implementation of MarginProbe for intraoperative margin assessment. Results: Utilization of MarginProbe produced a statistically significant relative reduction in re-excision of 71%. Total tissue volume removed was decreased from 69cc to 59cc, a 14% decrease in the MarginProbe group. These cases represent disease that was identified and removed through MarginProbe directed shaving, which would have otherwise remained unknowingly in the breast as residual disease. Conclusions: the 2014 Consensus Guideline of No Ink on Tumor to define positive invasive margin seeks to reduce national re-excision rates while consequently reducing cost to the health care system and improving quality of care and patient satisfaction. Multiple studies to date indicate a relative reduction in re-excision of 8-33% after adoption of the invasive margin guidelines. Implementing MarginProbe radiofrequency spectroscopy as standard of care further reduces rates of re-excision beyond those achieved with Consensus Guidelines alone, reaching low single-digit rates, and no increase in total volume of tissue removed. Future studies should seek to determine if this identification and removal of residual disease will have a positive effect on local recurrence rates. Secondary outcomes including grade and presence of lymphovascular invasion were also assessed. Pre-operative imaging assessment of axillary nodes is essential in patient counseling and operative planning. Clinicopathologic factors and surgical management were assessed for the entire cohort. We then compared trends over time between 2 groups: early group (diagnosed 2007-2013) and recent group (diagnosed 2014-2017). Continuous and categorical variables were compared using the Welch t-test and Chi-square test.