

Baha M. Sibai, MD
- Professor and Chair
- Department of Obstetrics and Gynecology
- University of Cincinnati College of Medicine
- Cincinnati, Ohio
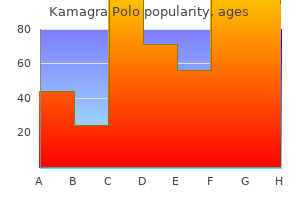
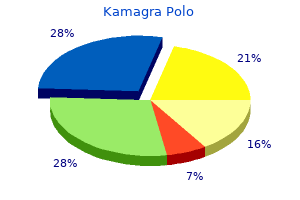
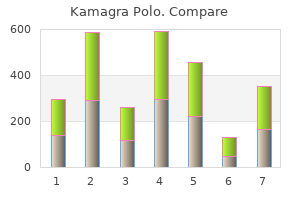
Finally best erectile dysfunction doctor discount kamagra polo 100 mg otc, the expert panel also showed that a large share of people who would benet from cholesterol reduction impotence yoga pose buy cheap kamagra polo online, by drug therapy or other means erectile dysfunction doctors in memphis tn order kamagra polo no prescription, have failed to 16 get appropriate diagnosis or treatment erectile dysfunction testosterone order 100 mg kamagra polo. The role for statin drug therapy has also expanded because it has proved difcult to reduce cholesterol substan17 tially by traditional means such as dietary changes. Statin Drug Competition and Marketing Developing drugs that reduce cholesterol and the risk of heart disease was a major medical breakthrough. Retail prices for the entire statin drug market have been very stable, increasing 19 only 7 percent in real terms between 1995 and 2000. Because these data do not reect private discounts and rebates from manufacturers to pharmaceutical benet managers or managed care organizations, prices are probably falling despite the surge of interest in these drugs. Monkman, Treating Dyslipidaemia in Primary Care: the Gap between Policy and Reality Is Large in the U. Product promotion, or marketing, is the most transparent and potentially most effective way for pharmaceutical rms to compete. In one prominent marketing strategy, called physician detailing, pharmaceutical representatives visit physicians, managed care organizations, health insurance companies, or afliated organizations such as pharmaceutical benet management rms to stress how their drugs can reduce health care or labor costs. On the other hand, pharmaceutical rms have limited experience in using broadcast advertising of prescription drug brands to motivate consumers to see their physicians about possible medical conditions. Some Empirics of Market Conditions Market data from 1995 through 2000 reveal the salient characteristics of the statin drug market and motivate systematic analyses of possible causal relations. As expected in a market for an effective new drug, demand has 23 been growing steadily (Figure 1). The growth in prescriptions decomposed into new and renewals (with brand switches recorded as new 24 prescriptions) was very similar to the growth in total pills dispensed. Although the trend in demand has been steadily upward, the trend in the promotion of statin drugs has been irregular. Figure 3 decomposes these into broadcasting (mainly television), popular print, medical journals, and physician detailing and shows that television advertising has become far more important since the rule change, while popular print advertising appears somewhat less important. Specically, we included a dummy variable to represent the 1998 presentation of preliminary results of a clinical trial that attracted considerable attention because it demonstrated that for many heart 26 disease patients, statin drug therapy was at least as effective as angioplasty. Because a Dickey-Fuller test revealed that the dependent variable was nonstationary, these models were estimated using rst differences (in logs). We also estimated models using alternative measures of demand 25 Pierre Azoulay, Do Pharmaceutical Sales Respond to Scientic Evidence Strategy 551 (2002), found that both medical research ndings and promotion increased the sales of anti-ulcer drugs. None of these regressions yielded signicant coefcients for any of the advertising variables. Marta Wosinska, Effects of Direct-to-Consumer Drug Advertising on Prescription Choice (Working paper, Univ. This may take a a few weeks to 6 months or more, with considerable variance among patients and perhaps among physicians. Investigating Other Possible Effects of Direct-to-Consumer Advertising Because consumers may not respond to advertising in a way that is easy to detect empirically, we explored alternative ways in which advertising could affect this market. For example, advertising could affect demand by inuencing consumers to visit their doctors, get checkups and diagnoses, and ultimately use a cholesterol-reducing prescription drug. New diagnoses can signal a treatable condition and lead to additional ofce visits. Figure 5 shows that total ofce visits for patients under treatment for high cholesterol have risen from roughly 1 million in 1996 to more than 2. However, they are likely to have overstated these effects because it appears that they did not detrend their sales and advertising data. It is therefore possible to characterize a process that has been growing during the past 4 years in which consumers visit the doctor, get a diagnosis, and, when diagnosed with high cholesterol, usually get a statin prescription. Advertising may therefore have an indirect effect on statin drug demand by inuencing people to visit their doctor for a checkup and diagnosis. A Dickey-Fuller test revealed that the visits variables were nonstationary, so we estimated models using rst differences (in logs). We specied advertising expenditures in several alternative ways including simple lags and 3-month and 6-month stocks. The consistent nding was that advertising expenditures had a statistically insignicant effect on ofce visits. In addition, if advertising were having a strong effect on ofce visits, one might expect that patients would be initiating requests for statin drugs. In the face of growing cholesterol-related patient visits and statin drug demand, it would strengthen our ndings that advertising has had a statistically insignicant effect on this growth if we could point to what has caused it. One relevant fact is that actual and potential patients can obtain objective evidence on the efcacy of statin drugs in reducing serum cholesterol. This nding is consistent with the idea that information is playing a role in the growth of the statin drug market. That information is presumably not from advertising, but instead from successful treatments that we speculate are being discussed among friends, coworkers, and the public 30 at large as well as among physicians. Given that the Scott-Levin data indicate that the average total cholesterol levels of existing cholesterol patients declined from about 240 to about 215 between 1996 and the end of 2000, it would not be surprising if patients were sharing their positive experiences with statin drug therapy. But advertising may be having a subtle effect by reinforcing 30 Fred Mannering & Clifford Winston, Automobile Air Bags in the 1990s: Market Failure or Market Efciency This nding is consistent with survey evidence indicating that patients pay attention to advertising for drugs they are using, which reminds them to rell prescriptions 32 and stick with their regimens, thereby improving compliance. For instance, it has been alleged that drug advertising is attracting people into the market who do not need the drug. Robert Dubois and others nd that although considerably more patients received lipid-lowering therapy from 1997 to 1999, the dis33 tribution of statin use by risk prole has remained stable. According to the Scott-Levin data, average cholesterol levels for newly diagnosed patients have remained essentially constant since 1996. Given the aging of the population, this suggests, and is consistent with ndings in the medical literature, that statin drugs are underused rather than overused. As noted, average statin prices have probably declined and certainly have not been inated by promotional expenditures, which have been running at only 6 percent of statin revenues. Calfee, Public Policy Issues in Direct-to-Consumer Advertising of Prescription Drugs, 19 J. This function of advertising was noted by Victoria Stagg Elliott, Questions Swirl around Drug Ads for Patients, Am. We found previously, however, that advertising did not have a statistically signicant effect on brand shares. Given that physicians play a dominant role in statin drug use and that many patients who could benet from these drugs are not using them, it is possible that the prescription requirement is having adverse effects.
Bee saliva (Royal Jelly). Kamagra Polo.
- How does Royal Jelly work?
- Dosing considerations for Royal Jelly.
- High cholesterol, asthma, hayfever, liver disease, pancreatitis, insomnia, premenstrual syndrome (PMS), stomach ulcers, kidney disease, bone fractures, skin disorders, baldness, boosting immunity, and other conditions.
- What is Royal Jelly?
- Are there safety concerns?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96509
Infertility Patients and their partner may need advice and appropriate referral for fertility management zma erectile dysfunction trusted 100 mg kamagra polo. Cardiometabolic risk Lifestyle modifcation to induce >5% weight loss in those who are overweight should be recommended vascular erectile dysfunction treatment cheap kamagra polo 100mg fast delivery. Poor glycaemic control at conception and early pregnancy is associated with increased risk of congenital abnormalities and frst trimester abortions erectile dysfunction grand rapids mi buy cheap kamagra polo 100 mg line. Both maternal and fetal complications are elevated when a pregnant woman has diabetes impotence vs erectile dysfunction generic kamagra polo 100 mg free shipping. Good glycaemic control can mitigate the risk of maternal and fetal complications and the likelihood of birth trauma, and reduce the risk of early induction of labour and need for caesarean section. With one exception, the advice in this section is also applicable to a patient with type 1 diabetes preparing for pregnancy with the management being restricted to insulin only. For example proliferative retinopathy may be worsened in pregnancy and, if present, should be treated. Women should be reassured that any reduction in HbA1c towards the individualised target is likely to reduce the risk of congenital malformations. Medications should be assessed on an individual basis, acknowledging the pregnancy risk classifcation and balanced against the beneft of continuing the medication during pregnancy and lactation. Safety of diabetes medications before and during pregnancy Consideration of the safety of current oral and or injectable diabetes therapies should be undertaken ideally before pregnancy is planned or urgently once pregnancy is confrmed. Consultation with local specialist services on an individualised medication regimen is advised in most cases. Metformin and sulphonylureas are not associated with an increase in congenital malformation or early pregnancy loss. Some oral agents such as the glitazones and gliptins may need to be ceased and insulin therapy instituted. Insulin Rapid-acting insulin analogues aspart and lispro may be safe to use during pregnancy. There is insuffcient evidence about the use of long-acting insulin analogues except for detemir insulin (a long-acting insulin analogue) which is now classifed as category A in pregnancy for patients with type 1 diabetes. Close surveillance for new diabetes complications and monitoring of existing complications should occur routinely. This is an appropriate time to address breastfeeding as well as review medications. In normal pregnancy there is a natural increase in hyperglycaemic hormones including cortisol, growth hormone, human placental lactogen, progesterone and prolactin levels. In pregnant women with abnormal glucose intolerance, however, the hyperglycaemic effects of pregnancy hormones is not adequately compensated. Potential maternal complications during pregnancy and delivery include preeclampsia and higher rates of caesarean delivery. For the neonate, complications include birth injuries, respiratory diffculty at birth, hypoglycaemia and jaundice. This usually includes nutritional therapy, exercise, blood glucose monitoring and insulin therapy. Maternal weight loss during pregnancy is potentially dangerous for the developing fetus and is not advised. Close cooperation with the obstetric team is advised to monitor both maternal and fetal welfare. Other contraceptive implants and intrauterine devices may also be an option on an individual basis. Men with diabetes are four times more likely to develop erectile dysfunction than men without diabetes. The prevalence in men aged over 40 years with diabetes may be as high as 50% and incidence increases by approximately 10% per annum. Men with diabetes are also affected by erectile dysfunction at an earlier age than men who do not have diabetes, with occurrence approximately a decade earlier. Failure to achieve erection may be due to psychological causes, macrovascular disease or pelvic autonomic neuropathy. An organic cause is more likely when there are other macroor microvascular complications. In addition, as a population/group/cohort, men with diabetes, (both type 1 and type 2), have been shown to have lower testosterone levels than men without diabetes. This may contribute to reduced libido and aggravate or exacerbate erectile dysfunction. In practice It is important to enquire about erectile dysfunction in the annual review (cycle of care) and to differentiate psychogenic from organic causes. Usually enquiring about spontaneous erections while asleep or in non-sexual situations will help. Phosphodiesterase inhibitors (sildenafl, tadalafl, vardenafl) starting with a low dose are available for men with erectile dysfunction who wish to resume sexual activity. If vasodilating nitrates are used, phosphodiesterase inhibitors can cause catastrophic and life-threatening hypotension, and are contraindicated. Other techniques such as intrapenile prostaglandin E1 (alprostadil) by injection, vacuum devices, or penile prostheses or implants may help. The help of a sympathetic specialist urologist should be sought for those considering penile injection with vasoactive agents (preparations now commercially available) or surgical treatment. Women with diabetes may also experience higher rates of sexual dysfunction than their non-diabetic counterparts. Genital infections including moniliasis and vulvitis, which may contribute to sexual dysfunction, are not uncommon in diabetes. Rates of depression, anxiety and psychological distress are higher in people with diabetes and may contribute to sexual dysfunction in men and women. In practice It is important to enquire about sexual problems in the annual review and to manage physical and emotional aspects. This plan should be Australian Diabetes provided reviewed at regular intervals Educators Association, 2006 Assist in development of a sick day care plan and preparation (174) None of a home sick day management kit for patients to use during Australian Diabetes provided episodes of sickness Educators Association, 2006 *Refer to Appendix A for an explanation of the Grade. A clear and specifc action plan ensures that patients can either self-manage or have access to their healthcare team for advice and early intervention, supervision and support. Pre-operative care is the same for both minor and major surgery, but blood glucose levels should be monitored intra-operatively (a prolonged procedure) and postoperatively for several days. Metformin can generally be recommenced 24 hours after major surgery provided that there has been no deterioration in serum creatinine.
Arginase deficiency Energy requirements will often be greater than normal because of low intakes both pre-diagnosis Arginase deficiency (Fig impotence cure food purchase discount kamagra polo on line. If the baby is being breast fed It is characterised by a progressive spastic tetraplethe mother should be encouraged to express until gia impotence effect on relationship safe 100 mg kamagra polo, seizures erectile dysfunction protocol food lists quality 100 mg kamagra polo, developmental regression and poor the baby is more stable generic erectile dysfunction drugs online buy kamagra polo 100 mg online, then breast feeding can be growth [256]. Arginase deficiency is treated with a low protein diet, sodium benzoate and phenylbutyrate. This Management of illness treatment should prevent further neurological During intercurrent illness, protein catabolism damage and may induce a partial recovery of skills may cause rapid accumulation of ammonia and over time [274]. Protein intake is All dietary nitrogen has the potential to be constopped temporarily and regular 2-hourly drinks verted to arginine, this source being considerably of glucose polymer are given. The usual doses of greater than the small amount of arginine that is sodium benzoate, phenylbutyrate and arginine are naturally present in protein. However, deaths the diet is monitored by regular measurements have been reported resulting from hyperammonof plasma ammonia, plasma arginine and the other aemic encephalopathy triggered by infection [274]. The aim is to maintain Sodium benzoate and phenylbutyrate should be plasma arginine levels at <200 mol/L (normal given orally or intravenously. In some bolites from either protein catabolism and/or lipolysis in disorders such as organic acidTable 17. A solution of glucose polyare well to ascertain what they will take and to mer is given as the main energy source because it is familiarise the parents with reconstitution of these simple to administer and is usually well tolerated. Fat emulsions can be added as an addithese drinks are convenient because they are ready tional energy source, but these may be less well to use, portable and can be stored for use in an tolerated, particularly in the child who is vomiting. This is easily performed in hospiTo reduce the period of fasting and optimise tal but may be more difficult at home. Too concentrated a solution of gluand more realistic targets should be considered. Dextrose 10% is be taught to make these drinks using handy scoop given by peripheral drip or more concentrated dexmeasurements. If oral or Treatment of intercurrent infections can be an enteral feeds cannot be re-established then an early anxious and difficult time for parents. To make resort to parenteral nutrition is indicated for some this easier, parents should be taught a three-staged disorders [278]; refer to specific disorders. If prolonged, malnutrihelp reduce episodes of metabolic decompensation tion may develop surprisingly rapidly. If subtle changes in behaviour are usually the earso, it may be necessary to increase protein intake liest signs of this and are most easily detected by temporarily when the child is well to compensate parents [281]. As the child improves normal diet is reintro2 If on reassessment the child has improved, the duced. Protein, whether from feed the parents should be taught to recognise signs or diet, is reintroduced by increasing the daily of encephalopathy such as disorientation and poor amount, providing one-quarter, half and threeresponsiveness, accompanied by a glazed look. They observed that ketones period (usually less frequently) to maximise energy were present during times of illness, but not in intake. If on feeds, additional glupatients as there is wide variation in how they cose polymer is added to the infant formula or low respond so that each should be assessed individuprotein tube feed to the same concentration as the ally. This reintroduction gested fluid volumes, feeding frequency and conperiod will be performed more rapidly over fewer tact telephone numbers. Juvela Low Protein Cinnamon Cookies 150 g these guidelines are also very useful for families Juvela Low Protein Orange Flavour Cookies 150 g when on holiday. Families can travel abroad, but it Juvela Low Protein Chocolate Chip Cookies 130 g is best they go to countries that have expertise in the Loprofin Low Protein Crackers (Savoury) 150 g management of metabolic disorders should the child Loprofin Low Protein Herb Crackers 150 g become unwell. Loprofin Low Protein Pasta Spirals 500 g Loprofin Low Protein Macaroni Penne 500 g Loprofin Low Protein Vermicelli 250 g Loprofin Low Protein Short Cut Spaghetti 500 g Appendix 17. Crystal *Milupa lp-drink 400 g structure of the catalytic domain of human pheny250 mL = half an exchange when made as lalanine hydroxylase reveals the structural basis for per instructions phenylketonuria. A European Contains approximately half an multicenter study of phenylalanine hydroxylase exchange per carton deficiency: classification of 105 mutations and a *Sno-Pro Drink 200 mL carton general system for genotype-based prediction of Contains half an exchange per carton metabolic phenotype. Human Burger mix phenylalanine hydroxylase mutations and hyperphenylalaninemia phenotypes: a metanalysis of Firstplay Dietary Foods Limited genotypephenotype correlations. Neuro23 Medical Research Council Working Party on Phenylogical deterioration in young adults with phenylketonuria. Information processing in patients with abnormalities in patients with treated hyperphenyearly and continuously-treated phenylketonuria. Pheny31 Burgard P Development of intelligence in early lketonuria in adulthood: a collaborative study. Regression of adult patients with phenylketonuria improve their neuropsychological deficits in early-treated phenyquality of life after introduction/resumption of a lketonurics during adolescence. Neuro47 Blau N, Erlandsen H the metabolic and molecular psychology of early treated phenylketonuria: spebases of tetrahydrobiopterin-responsive phenylalacific executive function deficits. Enzymatic contemporal syndrome in adolescents with optimally trol of phenylalanine intake in phenylketonuria. Dietary management of inborn errors of phenylalanine concentrations in phenylketonuria: metabolism. Tyrosine suppatients with phenylketonuria: effect of sample plementation in phenylketonuria: diurnal blood timing. Resting Disorders of Amino Acid Metabolism, Organic Acidaemias and Urea Cycle Defects 383 energy expenditure in children with phenylkeselenium-deficient phenylketonuric and hypertonuria. Effects amino acids as a parameter for catabolism in treated of a low selenium state in patients with phenylkephenylketonuria. Increased concentrations in 42 treated phenylketonuric chilrisk of vitamin B12 deficiency in patients with dren. Vitamin B12 deficiency in adolescents and young 86 Colome C, Artuch R, Lambruschini N et al. Fish oil supidation products before and after selenium suppleplementation improves visual evoked potentials in mentation. Potentially life-threatening cardiac dysrhythmia in 90 Giovanni M, Biasucci G, Agostoni C et al. Lipid staa child with selenium deficiency and phenylketus and fatty acid metabolism in phenylketonuria. Effects of iron availability as a possible cause of low serum long-chain polyunsaturated fatty acid supplemencarnitine concentrations in patients with phenylketation on fatty acid status and visual function in tonuria. Plasma phenylalanine concentrations are associated 92 Agostoni C, Verduci E, Massetto N et al. Long term with hepatic iron content in a murine model for effects of long chain polyunsaturated fats in hyperphenylketonuria.
Urbino Daza erectile dysfunction types buy cheap kamagra polo 100 mg online, and he was welcomed with special deference erectile dysfunction causes anxiety discount kamagra polo 100mg on-line, although he was not asked to sign the gold book for notable guests erectile dysfunction urology tests purchase kamagra polo mastercard. The fears regarding the meeting that had troubled Florentino Ariza since the previous afternoon vanished with the port he had as an aperitif erectile dysfunction urban dictionary order cheapest kamagra polo and kamagra polo. Because of everything that he said, Florentino Ariza realized that she had spoken to her son about him. She told him that they had been childhood friends, playmates from the time of her arrival from San Juan de la Cienaga, and that he had introduced her to reading, for which she was forever grateful. She also told him that after school she had often spent long hours in the notions shop with Transito Ariza, performing prodigious feats of embroidery, for she had been a notable teacher, and that if she had not continued seeing Florentino Ariza with the same frequency, it had not been through choice but because of how their lives had diverged. He thought that the world would make more rapid progress without the burden of old people. From the medical point of view, according to him, the proper age limit would be seventy. But until they reached that degree of charity, the only solution was nursing homes, where the old could console each other and share their likes and dislikes, their habits and sorrows, safe from their natural disagreements with the younger generation. Urbino Daza wanted to thank Florentino Ariza for the good companionship he gave his mother in the solitude of her widowhood, he begged him to continue doing so for the good of them both and the convenience of all, and to have patience with her senile whims. Urbino Daza had not noticed the inappropriateness of his prognostications, and he became enmeshed in a long series of explanations that only made matters worse. He was radiant, for he knew that sooner or later he was going to have another meeting like this one with Dr. The lunch had been very encouraging, not only in and of itself but because it showed him how simple and well received that inexorable request was going to be. Moreover, after their conversation at this historic lunch, the formality of a request was almost de trop. The staircase in his offices seemed the most dangerous of all to him because it was so steep and narrow, and long before he had to make a special effort not to drag his feet, he would climb it with his eyes fixed on each step and both hands clutching the banister. It had often been suggested that he replace it with one that was less dangerous, but he always put off the decision until next month because he thought it was a concession to old age. As the years passed, it took him longer and longer to walk up the stairs, not because it was harder for him, as he himself hurried to explain, but because he used greater and greater care in the climb. Urbino Daza, after the aperitif of port and half a glass of red wine with the meal, and above all after their triumphal conversation, he tried to reach the third stair with so youthful a dance step that he twisted his left ankle, fell backward, and only by a miracle did not kill himself. As he was falling he had enough lucidity to think that he was not going to die of this accident because the logic of life would not allow two men, who had loved the same woman so much for so many years, to die in the same way within a year of each other. He was put into a plaster cast from his foot to his calf and forced to remain immobile in bed, but he was livelier than he had been before his fall. When the doctor ordered sixty days of convalescence, he could not believe his misfortune. But when at last he walked again, his ankle still painful and his back raw, he had more than enough reasons to believe that destiny had rewarded his perseverance with a providential fall. The pain had eased and the medical prognosis was very encouraging, but he refused to accept the fatality of not seeing Fermina Daza the following afternoon for the first time in four months. Nevertheless, after a resigned siesta, he submitted to reality and wrote her a note excusing himself. He wrote it by hand on perfumed paper and in luminous ink so that it could be read in the dark, and with no sense of shame he dramatized the gravity of his accident in an effort to arouse her compassion. She answered him two days later, very sympathetic, very kind, without one word extra, just as in the great days of their love. He asked the operator to connect him with the three-digit number that he had known by heart since the first time he dialed it. The quiet voice strained by the mystery of distance, the beloved voice answered, recognized the other voice, and said goodbye after three conventional phrases of greeting. Florentino Ariza was devastated by her indifference: they were back at the beginning. Two days later, however, he received a letter from Fermina Daza in which she begged him not to call again. There were so few telephones in the city that all communication took place through an operator who knew all the subscribers, their lives, their miracles, and it did not matter if they were not at home: she would find them wherever they might be. In return for such efficiency she kept herself informed of their conversations, she uncovered the secrets, the best-kept dramas of their private lives, and it was not unusual for her to interrupt a conversation in order to express her point of view or to calm tempers. Despite her unimpeachable life, Fermina Daza was more careful now than ever of everything she said or did, even with her closest friends. So that she maintained her connection to Florentino Ariza by means of the anachronistic thread of letters. The correspondence back and forth became so frequent and intense that he forgot about his leg and the chastisement of the bed, he forgot about everything, and he dedicated himself totally to writing on the kind of portable table used in hospitals to serve meals to patients. They called each other tu again, again they exchanged commentaries on their lives as they had done once before in their letters, and again Florentino Ariza tried to mo ve too quickly: he wrote her name with the point of a pin on the petals of a camellia and sent it to her in a letter. This was, according to her, the reason for his haste and constant blundering as he evoked the past. She could not understand how a man capable of the thoughts that had given her the strength to endure her widowhood could become entangled in so childish a manner when he attempted to apply them to his own life. Now it was she who tried to give him new courage to face the future, with a phrase that he, in his reckless haste, could not decipher: Let time pass and we will see what it brings. His forced immobility, the growing lucidity of his conviction that time was fleeting, his mad desire to see her, everything proved to him that his fear of falling had been more accurate and more tragic than he had foreseen. For the first time, he began to think in a reasoned way about the reality of death. Leona Cassiani helped him to bathe and to change his pajamas every other day, she gave him his enemas, she held the portable urinal for him, she applied arnica compresses to the bedsores on his back, she gave him the massages recommended by the doctor so that his immobility would not cause other, more severe ailments. On Satur days and Sundays she was relieved by America Vicuna, who was to receive her teaching degree in December of that year. He had promised to send her to Alabama for further study, at the expense of the river company, in part to quiet his conscience and above all in order not to face either the reproaches that she did not know how to make to him or the explanations that he owed to her. He never imagined how much she suffered during her sleepless nights at school, during the weekends without him, during her life without him, because he never imagined how much she loved him. He had been informed in an official letter from the school that she had fallen from her perpetual first place in the class to last, and that she had almost failed her final examinations. Without realizing it, he was beginning to defer his problems in the hope that death would resolve them. The two women who took care of him, and Florentino Ariza himself, were surprised at how much he had changed.
Order kamagra polo 100mg free shipping. What is Erectile Dysfunction (in Hindi)- By Dr Praveen Tripathi.