

Todd Larabee, MD
- Assistant Professor
- Division of Emergency Medicine
- University of Colorado Denver School of Medicine
- Aurora, Colorado
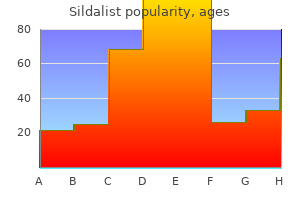
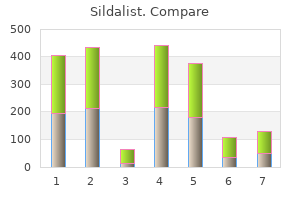
Diferent literature and review articles on Gymnema are studied about its phytochemical constituents and their antidiabetic and antioxidant activities erectile dysfunction after radical prostatectomy treatment options sildalist 120 mg fast delivery, parts use erectile dysfunction treatment centers in bangalore purchase discount sildalist line, method of use erectile dysfunction johns hopkins generic 120 mg sildalist, color erectile dysfunction internal pump order 120 mg sildalist otc, taste, duration of use, etc. The list of references of all relevant articles was also studied to include all reports and reviews related to the matter. Cultivation Gymnema sylvestre reproduces vegetatively through stem cuttings and sexually through seeds. Seeds are sown in the month of November and Figure 1: Chemical structure of the important bioactive molecules December and are harvested afer 8-9 months. In case of gymnemasaponins, anti-sweet activity is also developed due to the presence of Acyl group, so it is an aglycone part of saponin. Antidiabetic activities of various bioactive components are very much essential for Type 2 diabetes control (Table 1). Figure 2: Blood sugar reduction potential of diferent biocomponents of Gymnema sylvestre. Antioxidant like ascorbic acid neutralizes hydroxyl radicals, super oxide radicals thereby proving its antioxidant nature and also showing blood sugar uptaking abilities. Both antioxidant and antidiabetic function is very helpful in Type 2 diabetes treatment. Other antioxidants like Chemical Structure of Bioactive Compounds Terpenoid, Flavonoid, Cinnamic acid, Folic acid, Tannin, Phenol etc. In case of Gymnema sylvestre, gymnemic acids are triterpenoid gly- also perform antidiabetic as well as antioxidant activity. This is As antidiabetic components of Gymnema show antioxidant activities adorned with a sugar such as glucoronic acid and with various ester vice versa antioxidants also show their antidiabetic potential (Table 2). The agly- Based on various scientifc literature, it has been proved that Gymnema cone gymnemagenin is a D-glucoronide of hexa-hydroxytriterpene. Seven new dammarane saponins, named Gymnemasides i-vii Gymnema sylvestre and their mode of action. Flavonoids Gymnema sylvestre have 15 carbon skeleton structure that consists of two phenyl rings (A and Oleanane Hypoglycemic activity. Cinnamic acid is white crystalline organic Gymnemic acid Reduction of blood sugar because 41 compound which is highly soluble in organic solvent. It is classifed as an gymnemic acid molecules fll the unsaturated carboxylic acid. Another antioxidant, folic acid also called receptor location in the outer layer as Vitamin B9, is white and crystalline compound. It is also known as of intestine, thereby preventing sugar phenolic acid or pteroglutamic acid. Phenols are aromatic, white Gymnemasides (A-F) Inhibitory efects on increased level 42-44 crystalline compounds where hydroxyl group is attached with carbon of serum glucose. Essential Chemical Components of Gymnema sylvestre Gymnemic acidA1 Antisweet activity. Glucose Level Triterpenoidsaponin Hypoglycemic and anti 49 Proposed mechanism for the hypoglycemic action of gymnemic acid hyperglycemic activity. Gymnestrogenin) Gymnemagenin inhibits glucose on the intestine and stop glucose molecule from binding to the receptor absorption and thus prevent excess glucose absorption. Gymnemic acid binds to Pharmacognosy Journal, Vol 11, Issue 2, Mar-Apr, 2019 203 Laha and Paul. Ascorbic acid Neutralise hydroxyl, superoxide 53,54 and hydrogen peroxide radicals. Effect of herbal hypoglycemic on oxidative stress and antioxi- Nonacosane, Scavenging free radicals and 55,56 dant status in diabetic rats. A pharmacological pentatriacontane, fi and appraisal of medicinal plants with antidiabetic potential. Formulation of anti-diabetic Cinnamic acid, Folic acid, having reducing power ability. Reduction of blood glucose and Asian Journal of Pharmaceutical and Clinical Research. Oxidative stress and the use of Stimulation of insulin secretion antioxidants in diabetes. Management of diabetes mellitus: Could simultaneous targeting Inhibition of fi-amylase and of hyperglycemia and oxidative stress be a better panaceafi. Kerala Agriculture University Aromatic and Medicinal plant not so many research activities done on mode of actions of gymnema- research station Odakkali. Antidiabetic activity along with antioxidant potential of Gymnema (Asclepiadaceae): structures of gymnemosides A and B. Br have been reported till date due to the presence of favonoids, ceutical Bulletin. Triterpenoid saponins from Gymnema that biocomponents possess both antidiabetic and antioxidant activities sylvestre. Production of plant bioactive Triterpenoid saponins: elicitation strategies and target genes to improve increases day by day, more efective research and assessment or analysis yields. Two new favonol glycosides with exact active antidiabetic mechanism of action for human welfare from Gymnema sylvestre and Euphorbia ebracteolata. Characteristics of antisweet substances, sweet proteins and sweet- a sweet taste-suppressing polypeptide. Fecalsteroid excretion is increased activity relationships of triterpenoid derivatives extracted from Gymnema in rats by oral administration of gymnemic acids contained in Gymnema sylvestre leaves. Phytochemical and Pharmacological Properties ofGymnema sylvestre: An Important Medicinal Plant. A new penta- glucose homeostasis and metabolic parameters in arat model of metabolic hydroxy triterpene from Gymnema sylvestre leaves. Gymnemic acid, the antisaccharin principle of Gymnema sylvestre-Isolation and Impact of dietary poly-phenols oncarbohydrate metabolism. Santanu Paul is an Professor at the Department of Botany, University of Calcutta, India. He has experience in isolation and characterization of anti cancerous novel compounds from medicinal plants and looking at the mo- lecular mechanism of apoptosis induction. Suparna Laha is a Research Fellow at the Department of Botany, University of Calcutta, India. It focuses on the approaches and systems that are ideally in place to improve care for the majority of patients the majority of the time. Diabetes in pregnancy (gestational diabetes) is outside the scope of this guideline. Consider testing every 6 months if targets are consistently met and treatment and lifestyle are stable. Classifcation and Risk Factors Diabetes mellitus (diabetes in this guideline) is a complex chronic disease characterized by hyperglycemia due to defective insulin secretion, defective insulin action or both. Note: incidence uses three year moving average of 2011/2012 and prevalence uses 2012/2013 fscal year. Diabetes categories Type 1 Diabetes is primarily due to beta cell destruction, usually leading to total insulin defciency and is susceptible to ketoacidosis. The risk for developing type 1 diabetes is infuenced by Type 1 family history of type 1 diabetes and other autoimmune diseases. It may range from predominantly insulin resistance with relative insulin defciency to predominantly an insulin secretory defect with insulin resistance. Gestational diabetes does not exclude the possibility of preexisting, undiagnosed diabetes or glucose intolerance. Prevention fi Type 1 Diabetes Safe and efective therapies for the prevention of type 1 diabetes have not yet been identifed. Screening for type 2 diabetes should be performed every 3 years in individuals fi 40 years of age or those at high risk. Screen more frequently in people with additional risk factors for diabetes or at very high risk according to a validated risk assessment tool and test with either A1C ($12.
Educational resources from Diabetes Australia Membership of state and territory diabetes organisations provides access to a wide range of educational resources and support for people with diabetes beer causes erectile dysfunction discount sildalist express, their families and carers erectile dysfunction with diabetes type 1 sildalist 120mg low price, including information sheets in different languages available for free download from Cigarette consumption 0 (per day) Alcohol consumption fi2 standard drinks (20 g) per day for men and women protein shakes erectile dysfunction generic sildalist 120 mg fast delivery. Allowing for normal variation in test accuracy impotence lifestyle changes purchase cheapest sildalist, HbA1c results which range between 6. The number of people with type 2 diabetes is growing, most likely the result of rising overweight and obesity rates, lifestyle and dietary changes, and an ageing population. Within 20 years, the number of people in Australia with type 2 diabetes may increase from an estimated 870,000 in 2014, to over 2. The most socially disadvantaged Australians are twice as likely to1 develop diabetes. The early identifcation and optimal management of people with type 2 diabetes is therefore critical. General practice has the central role in type 2 diabetes management across the spectrum, from identifying those at risk right through to caring for patients at the end of life. We would also like to acknowledge the contribution of the previous editorial panel (Dr Pat Phillips, Dr Peter Harris, Dr Linda Mann and Ms Carole Webster), whose dedication and commitment to previous editions has been instrumental to the success of these guidelines. Type 2 diabetes is a largely preventable, chronic and progressive medical condition that results from two major metabolic dysfunctions: insulin resistance and then pancreatic islet cell dysfunction causing a relative insulin defciency. In the individual, these occur due to modifable lifestyle-related risk factors interacting with genetic risk factors. The concept of patient-centred care incorporates the patient experience of care and patients as partners in their healthcare. The recommendations tables include the reference or source of each recommendation, and the grade of recommendation. In cases where these are not available or current, results of systematic reviews and primary research studies have been considered to formulate the overall recommendation. Information specifc to the Aboriginal and Torres Strait Islander population is highlighted in boxed text. Recommendations in some areas are different for Aboriginal and Torres Strait Islander patients. It is therefore important to identify, record and report the Aboriginal and Torres Strait Islander status of patients. It requires a coordinated interaction between patients, healthcare providers and the healthcare system with a focus on improving the patient experience and outcomes throughout the continuum of care. For example, comprehensive care for diabetes starts with prevention: through timely identifcation of at-risk individuals, education and support, it is possible to prevent or delay the onset of type 2 diabetes. Owners of a general practice (and others involved in its corporate governance) play an active role in developing these systems by cultivating a culture focused on clinical quality and patient-centred care. Primary care is the central component of care across the spectrum of patients with diabetes: those dealing with a new diagnosis, those managing (often multiple) medications, those with complications of diabetes and multimorbidity, through to patients at the end of life. These programs bring together healthcare teams, evidence-based guidelines, useful support tools and good systems to support patients throughout their journey. General practices can access the Australian Government system level incentives to support diabetes care. Patients have experienced improvements in process and clinical outcomes with these management plans and team care arrangements. See Appendix B: Accessing government support for diabetes care in general practice. An effective system to achieve this needs to combine educated and engaged patients with a range of healthcare providers using good communication and information technology. Roles within a general practice team are not mutually exclusive, and clear guidance is required to identify the team member primarily responsible for key activities. Teamwork success may be supported by workfow charts for coordination and management of structured care programs (care planning). Decision support Accessible guidelines for diabetes management and associated issues. Clinical information systems Structured diabetes care programs require good information management systems (registers, recalls and reminders) combined with risk factor, complication assessment management and comorbidity strategies. Management plans are most effective when they involve a team care arrangement and are reviewed regularly. Several studies have shown that computerised recall systems, monitoring and reminding patients and practice team members about appointments, investigations and referrals improves diabetes care. Combining a reminder system with a practice register ensures that the reminder system is both systematic and targeted. This can prevent patients with diabetes General practice management of type 2 diabetes 7 missing out on basic care such as screening for retinopathy (30% not screened) and foot care (50% not checked every 6 months). Depending on the complexity of individual patient needs, structured recall may occur on a 3- to 12-month basis. Another example is where a structured recall may ensure that all necessary pathology tests are completed before the next practice visit by the patient. Self-management support the aim is to facilitate skills-based learning and patient empowerment. Diabetes self-management education can target medication education and compliance, goal setting, foot care and interpretation of laboratory results. Using practice data to identify areas in need of improvement is one way to achieve this. Clinical audit software tools are widely available to assist practices to evaluate clinical outcomes for patients with diabetes. Audit information can be used to improve management of patients with diabetes on many levels. Four of these indicators are relevant to diabetes care: Indicator Description number 1 Practice infrastructure to support safety and quality of patient care 5 Assessment of absolute cardiovascular risk 12 Screening for retinopathy in patients with diabetes 13 Screening for nephropathy in high-risk patients (including diabetes) Use of clinical indicators to assess care is advised but entirely voluntary. Clinical context Type 2 diabetes is the most common form of diabetes in Australia, although many cases remain undiagnosed. Note that the score may overestimate the risk of diabetes in those younger than 25 years and underestimate the risk in Aboriginal and Torres Strait Islander peoples. In practice Screen for undiagnosed diabetes in individuals at high risk25,26 (see Box 1).
Blinding is more important for less objec- tive result measurements erectile dysfunction pills cost purchase 120mg sildalist amex, such as pain or quality of life erectile dysfunction protocol book pdf discount sildalist 120 mg free shipping. Blind study: A study where some of those involved do not know which person is receiving one treatment or another causes juvenile erectile dysfunction order 120mg sildalist with visa, or placebo hot rod erectile dysfunction pills buy discount sildalist on-line. Treatment concealment is used to prevent the results of the research being "infuenced" by the placebo effect or by the bias of the observer. To correctly eval- uate the blinding, it is necessary to know who in the study has been blinded (patients, researchers, health professionals, results and/or statistic awarders). Cohort study (synonyms: follow-up, inci- dence, longitudinal study): An observational study where a defned group of people (the cohort) is monitored in time and where the results or outcome are compared between the subgroups of the cohort that were or were not exposed (or exposed to different levels) to an intervention or another factor of interest. The measurement of association that is used in these studies is relative risk and absolute risk. As a random distribution is not used, a pairing or a statistical alignment should be used to guarantee that the comparison groups are as similar as possible. Bone densitometry: Non-invasive diagnostic tests that measure the bone mass in differ- ent parts of the skeleton, by means of techniques that may or may not use ionising radiation, are included in this defnition. Ionising techniques include those that use gamma rays, such as sim- ple photonic densitometry, dual photonic densitometry, neutron activation analysis and Compton radiation count; these last two are still in experimental phase. Caregiver: A person that provides unselfsh and voluntary support to people affected, who either live with the patient or else devote part of their time (over 20 hours a week) to caring for the patients. Case and control study (synonyms: case control study, case referent study): Observational epidemiological study in which individuals with a certain disease or outcome of interest (cases) are selected, and compared with an appropriate control group without the disease or outcome of interest (controls), or in relation to the prior exposure of possible risk factors associated with the disease. The relationship between a factor (intervention, exposure or risk factor) and the outcome of interest is examined by comparing the frequency or level of this factor in the cases and in the controls. Case and con- trol studies are retrospective, as they are always developed looking backward in time. For example, to determine if thalidomide was the cause of birth defects, a group of children with these malformations (cases) was able to be compared with a group of children without those defects (controls). Then, both groups were compared with respect to the proportion of those ex- posed to thalidomide in each one of them by their mothers taking that medication. Clinical series (also case series): Uncontrolled observational study that includes an inter- vention and a result of more than one person, where the experience with a group of patients with a similar diagnosis, with no comparison group, is described. Clinical trial (synonyms: therapeutic trial, intervention study): Experimental study to eval- uate the effcacy and safety of a treatment or other intervention. This general term includes ran- domised controlled clinical trials and controlled clinical trials. It is the most commonly used design to assess the comparative effcacy of the drugs. Cochrane review: Systematic and updated review of the most reliable scientifc evidence about the benefts and risks of health care. This is also the name given to a systematic review carried out according to the Cochrane Collaboration methodology and published in the Cochrane Library. The Parent database (database of reference) is comprised of review modules sent by the Review Collaborator Groups that are registered in the Cochrane Collaboration. The re- views included in one of the modules that comprise the Parent database are reviewed by the publishing team of the Review Collaborator Groups, as described in the different modules of each one of the groups. The reviewers follow the guidelines published in the Cochrane Manual for Reviewers. Cochrane reviews are prepared using the Review Manager (Revman) software, provided by the Collaboration and that adapts to a structured format. Margin of values within which the real value of the population can be expected with a certain likelihood. Specifc likelihood is called level of confdence, and the endpoints of the confdence interval are called confdence limits (upper and lower). Confdence intervals with a likelihood of 95% are generally used, although sometimes 90% or 99% are used. Note: confdence intervals represent the likelihood of committing random errors, but not committing systematic errors (biases). Consistency: this refers to the extent to which the results obtained by a measurement pro- cedure can be reproduced. Lack of consistency may arise from differences between observers or measurement instruments, or due to lack of stability of the variable measured. Control: In clinical trials that compare two or more interventions, a control is a person from the comparison group that receives a placebo, no intervention, traditional care or any other type of service. In case and control studies, a control is a person in the comparison group without the disease or outcome of interest. In statistics, controlling means adjusting or bearing in mind the external infuences or ob- servations. Programmes aimed at reducing or eliminating a disease are also called control, especially when applied to transmissible diseases (infectious). Controlled clinical trial: this refers to a study that compares one or more intervention groups with one or more comparison groups (control). Although not all the controlled studies have a random distribution, all the clinical trials are controlled. The measurement used is the correlation coeffcient (r) that quantifes the linear relationship between exposure and disease. Cost effectiveness analysis: Assessment of the results obtained in terms of increase in therapeutic beneft derived from the extraordinary costs. The result is expressed as a ratio between cost and effectiveness, measuring the costs in monetary units and the benefts in terms of effectiveness units, such as life years gained. Crossed clinical trial: Type of randomised clinical trial in which the individuals receive two or more treatments in successive periods that have been randomly determined, enabling each indi- vidual to carry out his/her own control. On reducing variability, these trials are more effcient and their statistical power is greater. To prevent the effects of the frst treatment of the sequence from being expressed in the second period, lavage periods are usually included between treatments to avoid residual effects. Cross-sectional study or prevalence study: Study that examines the relationship between the diseases (or other health characteristics) and other variables of interest that might exist in a defned population at a specifc moment in time: the temporary cause-effect sequence cannot nec- essarily be established in a cross-sectional study. Delphi method: Qualitative research technique of consensus, aimed at a comprehensive and dynamic explanation, and the analysis of certain phenomena with the purpose of generating ideas, sharing experiences and sensing tendencies for the future. It purports to analyse a reality, reaching agreements on the phenomena regarding which there is no conclusive information. It is especially useful when working with very subjective elements, when it is diffcult to determine their intrinsic value. The problem is formulated and a panel of trained experts is selected to contribute to the study with their knowledge and experience. The questions that will be submitted to study are determined and posed to the members of the panel. An anonymous ques- tionnaire posed to the members of the panel in successive rounds until a consensus is reached. The study concludes with the preparation of a report containing the fnal results of the survey. Firstly, evalu- ate the impact of one or several diagnostic strategies on clinical decisions or on outcome in pa- tients. This assessment is carried out by clinical trials or non-experimental comparative studies. The second objective, traditionally more frequent, is to determine the diagnostic capacity of a test (capacity to classify a person as healthy or sick). Its design is based on a comparison between the test that is studied and the gold standard, which are applied to a group of patients, assessing the results in terms of sensitivity, specifcity, predictive value or odds ratios. Double blind: Clinical trial where neither the participants nor the researchers are aware of which intervention has been administered to the participants. The purpose of blinding the partici- pants (both receivers and suppliers of the care) is to prevent performance bias. Effect estimation (synonym: therapeutic effect): In studies on the effects of health care, this is the name given to the relationship observed between an intervention and an expressed outcome, for example, such as the number of patients needed to treat, odds ratio, risk difference, relative risk, standardised mean difference or weighted mean difference. Effectiveness: Extent to which a diagnostic, preventive or therapeutic intervention when ap- plied in normal practice and in non-experimental conditions, achieves a benefcial result.
Smaller biopsies obtained via a transjugular approach as well as smaller biopsy gun needle biopsies are discouraged impotence yohimbe cheap sildalist 120 mg free shipping. Transbronchial or other lung biopsy with mycobacterial times-weekly amikacin or streptomycin early in therapy is histopathologic features (granulomatous infiammation or recommended causes to erectile dysfunction buy sildalist american express. Rifabutin se erectile dysfunction diabetes uk purchase sildalist now, necessitate the institution of therapy erectile dysfunction va disability buy generic sildalist 120mg line, which is a decision 300 mg/day is also effective but less well tolerated. Specimens should be cultured on both liquid no drug regimens of proven or predictable efficacy for and solid media. Multidrug regi- ditions and/or lower incubation temperatures include mens that include clarithromycin 1,000 mg/day may cause M. Surgical debridement may also be an essary including extended antibiotic in vitro susceptibility important element of successful therapy. Work focused around the International previous statements, including advances in the understanding of Working Group on Mycobacterial Taxonomy. By its very nature, this technique in this document, as well as the capacity for updating information limited identification of new species. The dramatic change in mycobacterial taxonomy came with Large gaps still exist in our knowledge. The search for evidence included hand- of isolates of clinical disease that cannot be identified with com- searching journals, reviewing previous guidelines, and searching mercial nucleic acid probes. The recommendations are rated on the basis consequence of newer identification techniques that are capable of a system developed by the U. Human disease is suspected to be acquired ratory were pulmonary, whereas 3% were lymph node and 3% from environmental exposures, although the specific source of were skin/soft tissue isolates (19). The most frequently reported potentially pathogenic States, rising rapidly between the ages of 1 and 12 years, then species and corresponding report rates over the 4-year period appearing to plateau (14). For diagnostic purposes, it may be necessary to collect multiple respiratory specimens on separate Body Morphotype days from outpatients. Overnight shipping with refrigerants such bronchiectasis have similar clinical characteristics and body type, as cold packs is optimal, although mycobacteria can still be sometimes including scoliosis, pectus excavatum, mitral valve recovered several days after collection even without these mea- prolapse, and joint hypermobility (27). The longer the delay between collection and processing, teristics may represent markers for specific genotypes that affect however, the greater is the risk of bacterial overgrowth. In addition, the optimal methodology for sputum induction ercept are effective antiinfiammatory agents and lead to rela- in this setting has not been determined. It is also important to perform appropriate clean- Infections with mycobacteria and fungi are seen with all three ing procedures for bronchoscopes that include the avoidance of agents, but significantly more with infiiximab than etanercept. If a swab is used, the bacteria isolated by culture are less likely to have positive smears swab should be saturated with the sampled fiuid to assure an (50). When submitting tis- sue, the specimen should not be wrapped in gauze or diluted in Culture Techniques liquid material. If only a minute amount if tissue is available, All cultures for mycobacteria should include both solid and broth however, it may be immersed in a small amount of sterile saline (liquid) media for the detection and enhancement of growth (43). However, broth media cultures alone may not be satisfactory because of bacterial overgrowth. Cultures in broth media have Blood a higher yield of mycobacteria and produce more rapid results Several commercial mycobacterial blood culture systems for than those on solid media. Tissue samples or fiuids from normally based media, such as Lofiwenstein-Jensen agar or agar-based me- sterile sites do not require decontamination. The agar-based ground aseptically in sterile physiological saline or bovine albu- media may also be used for susceptibility testing. Most clinically significant slowly growing myco- on microscopic examination of stained smears. Environmental bacteria grow well on primary isolation at 35 to 37 C with the contamination, which usually involves small numbers of organ- exception of the following: the newly described M. Previous which requires temperatures from 22 to 30 C for several weeks studies have indicated that specimens with a high number of and only grows at 37 C in liquid media, M. Recent studies skin, joint fiuid, and bone specimens should be cultured at 28 have shown, however, that identification using only conventional to 30 C and at 35 to 37 C. Optimal recovery of all species may biochemical analysis is both time consuming and increases turn- require duplicate sets of media at two incubation temperatures. Rapidly growing mycobacteria usually which form colonies on subculture in 7 days or fewer, are re- grow within 7 days of subculture. Supplemented culture media and special culture condi- molecular methods, must be used. Therefore, currently used in many clinical laboratories (AccuProbe; Gen- identification of most mycobacterial isolates to the species level Probe, Inc. Testing can be performed using isolates from solid cian and the laboratorian and in the event that a specific labora- or liquid culture media and identification of these species can tory does not have the necessary technology for species identifi- be achieved within 2 hours. However, some taxa may require additional ing the need for speciation of that isolate. The controversy to all organisms (conserved regions) and also areas where nucle- primarily stems from the observation that, unlike M. In addition, no interstrain nucleotide sequence Susceptibility breakpoints have been defined in the laboratory difference value that unequivocally defines different species has to distinguish populations of mycobacteria that are labeled sus- been established for mycobacteria (48). One of the major and clarified, the clinician should use in vitro susceptibility data limitations of this system, however, is that the MicroSeq database with an appreciation of its limitations and with the awareness has only one entry per species (generally the type strain) (61). Although the caveat that each laboratory must validate each method for not routinely recommended, this differentiation may be each species tested, and quality control and proficiency testing important epidemiologically and, in the future, therapeuti- requirements should be enforced. Isolates from patients who previously received macrolide to facilitate identification of M. Communication between the clinician and laboratorian macrolide-containing regimens who relapse or fail after 6 is essential for determining the importance and extent of months of macrolide-containing therapy. Routine susceptibility testing of this species is macrolide-containing regimens for patients with dissemin- not recommended (43). Until further data are available, the isolate is found on subsequent testing to be macrolide resistant. If the isolate proves to be rifampin resistant, suscepti- species that are macrolide resistant. Susceptibility testing of these species is difficult even with multiple cultures of the same strain (43). There are no current recommendations for one specific clude sputum production, fatigue, malaise, dyspnea, fever, he- method of in vitro susceptibility testing for fastidious moptysis, chest pain, and weight loss. Evaluation is often complicated by symptoms caused by coexisting lung diseases, such as bronchiectasis, chronic obstruc- 7. Physical findings are nonspecific and refiect underlying pul- monary pathology, such as bronchiectasis and chronic obstruc- tive lung disease. Pulsed-field gel electrophore- sis (nodular/bronchiectatic disease) (see the online supplement). These biopsies are performed because of the small size of the tissue findings correspond histopathologically to bronchiectasis, bron- sample) but demonstrates mycobacterial histopathology features chiolar and peribronchiolar infiammation, and granuloma for- (without a history of other granulomatous or mycobacterial dis- mation (94). Unfortunately, A plain chest radiograph may be adequate for evaluating many antigenic epitopes are shared by different mycobacterial patients with fibrocavitary disease. A single positive sputum culture, especially with a small number of organisms, is generally regarded as indetermi- 1.
Order sildalist 120mg with amex. Side Effects of Viagra in Hindi | By Ishan.