
Danijela Jelovac, M.D.
- Assistant Professor of Oncology

https://www.hopkinsmedicine.org/profiles/results/directory/profile/5503711/danijela-jelovac
Immune modulating additives have been an active area of nutrition research Protein: 4 antibiotics with penicillin order 200mg doxycycline. Glutamine has been associated with increased mortality in multi-system organ failure patients antibiotic beginning with c purchase generic doxycycline on-line. Total calorie need=1784-11(A)+5(W)+244(S)+239(T)+804(B) are only able to get the nasoduodenal feeding tube into the a infection rates in hospitals discount 100mg doxycycline with amex. These formulas may underestimate the metabolic needs of patients with certain underlying disease processes antibiotics for uti macrobid cheap 200mg doxycycline with amex. Enteral nutrition is always preferred to parenteral nutrition if no contra-indications exist. Decreased infection rate in patients on enteral nutrition and estimated stress level. Monitoring gastric residual volume for tolerance of tube feeding is controversial 1. Caution advised with gastric feedings in patients with gastric pathology Total Parenteral Nutrition (ie:Gastroparesis, gastric outlet obstruction, gastric stula) A. Reserved for patients who require long term enteral access surgery may improve outcomes b. Liver complications include transaminitis, cholestasis, steatosis, steatohepatitis, brosis, and cirrhosis 1. The appropriate time frame to start parenteral nutrition remains controversial if a Is there utility in monitoring gastric residual volumes Late parenteral nutrition (8 days) has been shown to be associated with fewer complications than early initiation (48 hours). If hemodynamically compromised, should hold enteral nutrition until fully resuscitated and stabilized 3. Triglycerides days then advanced to goal versus starting at 25cc/hr and advancing to goal as 5. Full feeding group had increased emesis, gastric residuals, use of prokinetic agents, higher glucose, and more constipation 7. Common practice is to initiate enteral feeds at 30% calorie goal for 24 hours then increase by 10-15cc/hr every six hours as tolerated H. Patient complaints of pain, gastric distention, atus, radiographic evidence of 118 5. Altered mental status including gait disturbances and paresthesias After 10 days on the ventilator, he has been deemed 6. Monitor serum phosphate levels with repletion often necessary mechanical ventilation and potentially extubated. On numerous attempts at weaning, he becomes tachypneic and this chapter is a revision of the previous versions by R. What nutritional factors may be playing into the dif culty weaning from the ventilator and how might you quantify them American Society for Parenteral and Enteral Nutrition Board of Directors: Clinical guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients, Nutrition Monitoring 2009. Metabolic cart provided within 24 h of injury or intensive care unit admission, signi cantly reduces mor tality in critically ill patients: a meta-analysis of randomized controlled trials. Patient must be metabolically stable domized Trial of Glutamine and Antioxidants in Critically Ill Patients. Reignier J, Mercier E, Le Gouge A, Boulain T, Desachy A, Bellec F, et al: Effect of Not b. End-tidal carbon dioxide per a given time is measured Monitoring Residual Gastric Volume on Risk of Ventilator Associated Pneumonia in Adults Receiving Mechanical Ventilation and Early Enteral Feeding: A Randomized Control Trial. Respiratory quotient is calculated versus Late Parenteral Nutrition in Critically Ill Adults. Overfeeding leads to dif culty weaning from the ventilator due to increased carbon dioxide production Refeeding Syndrome A. As feeds are initiated, there is an increase in serum insulin levels which shifts phosphate intracellularly and leads to a precipitous decline in serum phosphate D. Laboratory data is notable for acute pancreatitis have a mild self-limiting elevated amylase and lipase values. The release of activated pancreatic enzymes leads to auto-digestion of the pancreatic parenchyma resulting in in amation, microvascular injury, and necrosis. Activated enzymes may also enter the systemic circulation causing endothelial injury and activation of the in ammatory and coagulation cascades resulting in distant organ damage. Local complications should be suspected when, in the course of the disease, there is a recurrence of the abdominal 1. Severity pain, secondary peak in the pancreatic enzymes, aggravation or development of new a. Infected necrotic pancreatic tissue is presumed when extraluminal gas is identi ed iii. An acute peripancreatic uid collection (typically found in interstitial Changes in pancreas and peripancreatic tissue 2 pancreatitis) b. An acute necrotic collection de ned as an area of non-viable pancreatic or Single uid collection 3 peripancreatic parenchyma in the early stage of the disease before demarcation. A walled-off necrosis is a well-organized collection of heterogeneous liquid and 30-50% 4 non-liquid necrosis in a well de ned capsule more than 4 weeks after disease onset. The term pancreatic abscess has been abandoned in the current classi cation, 2 Total Score 0-10 replaced by the more contemporary term infected (peri)pancreatic uid collection. Unit have been established by a multidisciplinary international consensus conference. There is a lack of correlation between the degree of elevation of the amylase and lipase, and the clinical severity of the disease. Infection of necrotic pancreatic tissue is unusual in the rst week of disease scans 4 onset. The initial assessment of the severity of acute pancreatitis is based on the clinical of morbidity and mortality. Clinical outcomes are improved by delaying surgery more than 4 the rst week of disease onset, although there is some controversy surrounding weeks from disease onset. A recent meta-analysis suggests that prophylactic antibiotic use is not necrotic and non-necrotic tissue. Early intervention carries the risk of seeding the associated with a signi cant reduction in infected necrotic tissue, requirement for sterile necrotic tissue with microorganisms and incomplete debridement with the need surgery, or mortality. However, there was a signi cant reduction in the hospital length for further surgery. Signi cant clinical deterioration with high suspicion for infection of necrotic necrosectomy (debridement) with placement of large bore drains. With this approach, tissue (usually after 10-14 days) should prompt initiation of broad spectrum antibiotic viable pancreatic parenchyma may inadvertently be removed resulting in exocrine therapy. Rapid de-escalation should occur after return of culture data and antibiotics pancreatic insuf ciency and diabetes mellitus. For well-contained, well-de ned collections, less invasive techniques including f. The initial antibiotic therapy should be directed towards Gram-negative bowel percutaneous drainage, endoscopic (transgastric) drainage, and minimally invasive ora with good penetration into pancreatic tissue (ie, carbapenems, uoroquinolones, retroperitoneal necrosectomy may be used.
Ventriculomegaly antibiotic withdrawal symptoms buy doxycycline canada, (Q038) & Unspecified Congenital Hydrocephalus infection en la sangre doxycycline 200 mg for sale, (Q039) Congenital ventriculomegaly may not be due to fluid circulation abnormalities infection in lymph nodes buy doxycycline 200 mg on line, but should be reported if the size of the ventricles is 15 mm or more bacteria helicobacter pylori espaol order doxycycline online pills. For less severe prenatally detected ventriculomegaly (10-14 mm) it is recommended to follow the case until further imaging and a final diagnosis has been found postnatally. Ultrasound detection of a defect in the corpus callosum is difficult and requires a very detailed examination. Reduction Anomaly of the Cerebellum, (Q0432) Classification systems for malformations of the cerebellum are varied and are constantly being revised as greater understanding of the underlying genetics and embryology of the disorders is uncovered. The prognosis of this developmental disorder is highly dependent on the underlying disorder. It is generally considered to be an encepholoclastic lesion originating in the third trimester because of severe ischaemic insult(s) due to widespread vascular occlusion, infections or prolonged severe hydrocephalus. The prognosis is grave and with prenatal diagnosis pregnancy termination is an option. Congenital heart defects are those gross structural abnormalities of the heart or intra-thoracic vessels that are of actual or potential functional significance. They are one of the most important causes of infant morbidity and mortality and continue to constitute an important cause of disability and death in adult life. There is a large body of evidence emerging on the genetic and non-genetic risk factors for congenital heart disease. Other determinants, (some of which are potentially modifiable), include maternal diabetes, therapeutic and non-therapeutic drug exposure and lifestyle characteristics. Additional views including visualization of both left and right outflow tracts are recommended to improve diagnostic ascertainment. This detection rate must be viewed with some caution because the cardiac lesions may not have been the defining feature for cases where they are classified in the secondary position. Looking only at the 22 cases where a primary diagnosis of severe cardiac anomaly was made, a prenatal detection rate of 50% is calculated, (n=11), which is disappointing. Genetic disorders and teratogens have been implicated in aetiology, (including maternal diabetes). Other associated cardiac anomalies include mitral atresia, aortic arch anomalies and almost complete absence of the interventricular septum creating a single ventricle. Up to 30% of cases are associated with chromosome 22q11 deletion, (Di George), syndrome. The three-vessel view will be abnormal because the pulmonary artery lies below the aortic arch. The right atrium is connected to the morphological left ventricle which gives rise to the pulmonary trunk. Instead a common atrioventricular valve bridges the defect and there is loss of the normal differential insertion seen at the crux on the four chamber view. Atrioventricular septal defects are one of the most common forms of heart disease seen in prenatal life. The scan appearance is one of a single valve opening into both ventricular chambers. Prognosis depends on the presence of other abnormalities but as an isolated lesion long-term prognosis following correctional surgery is generally good. This type of defect is often associated with extra cardiac defects and chromosomal disorders, particularly Trisomy 21. However prenatally only three features are reliably seen: right ventricular hypertrophy may not be evident until the latter stages of pregnancy or indeed early neonatal life. This is done by ensuring that there is continuity between the left ventricle and aortic outflow. The abnormality may also be suspected when there is difficulty identifying the right outflow tract owing to pulmonary stenosis or atresia. Extra-cardiac defects, chromosomal anomalies and genetic conditions, (particularly 22q11. Aortic Valve Atresia or Stenosis, (Q224) this is a narrowing at the level of the aortic valve. It is rarely associated with extracardiac or genetic causes and is an evolving lesion, progressive during pregnancy. Approximately 10% of cases are associated with a chromosomal abnormality, usually Trisomy 13, Trisomy 18 or Turner syndrome. In severe cases the four-chamber view is already abnormal in the second trimester. The aorta is extremely hypoplastic and its origin and course are difficult to define. The mitral valve fails to open and there is no demonstrable flow from the left atrium to left ventricle on colour flow Doppler. Compensatory dilatation of the right ventricle and pulmonary trunk may be present. The most reliable way to assess the aortic arch is in the transverse view in the upper thorax. However, visualization of the aortic arch in longitudinal section is not a usual component of the routine prenatal ultrasound scan. In this view the aortic arch is smaller than normal and smaller than the arterial duct. There may be disproportion between the left and right ventricles and between the aortic arch and pulmonary trunk. However, this is not a reliable diagnostic feature as a slight discrepancy in size between left and right ventricle will be seen in a healthy third trimester fetus. Coarctation of the aorta is accompanied by extra-cardiac anomalies in 25% of cases. Typical anomalies include those whose embryonic development coincides with the timing and location of aortic arch development and include upper gastrointestinal tract anomalies such as oesophageal atresia and diaphragmatic defect. A total of six cases of coarctation of the aorta were diagnosed in 2015-2016, the majority, (n=4), had the abnormality coded in the primary position. Prenatal diagnosis is extremely difficult in the absence of an associated cardiac abnormality. A persistent left superior vena cava may be seen in transverse section directly adjacent to the left atrium on the four chamber view or as a 4th vessel to the left of the pulmonary trunk on the three-vessel view. Individuals with heterotaxy are broadly stratified into subsets of asplenia/polysplenia syndrome or isomerism of left/right atrial appendages. This form is typically associated with more severe cardiac defects and two tri-lobed lungs with short bronchi. The defects are categorized according to position as peri-membranous, doubly commuted sub-arterial and muscular. Ventriculo-septal defects may occur in isolation but are commonly associated with extra-cardiac and chromosomal abnormalities. In mesocardia the heart is centrally located in the chest, (the cardiac axis pints to the midline). Newborn infants are obligate nose breathers and bilateral choanal atresia is noted at birth by the absence of nose-breathing despite inspiratory effort and variable cyanosis. It was also felt likely that the pregnancy had initially been a twin gestation with a large but empty second sac. The trachea, filled with fluid, is visible in the coronal plane on antenatal scan. However, whilst the echogenic tracheal cartilage rings can be delineated from the less echogenic surrounding tissue and echo free lumen, a prenatal diagnosis of tracheal stenosis is therefore unlikely.
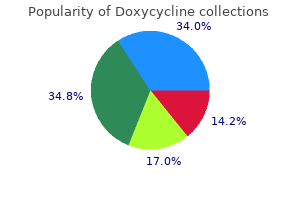
Purchase genuine doxycycline. Eco-Friendly and Zero Waste | Q-tips // Cotton Buds // Cotton Swabs.

Dysphagia or stridor (respiratory insufficiency) antibiotic resistance the need for global solutions discount doxycycline 200mg mastercard, or both infection in tooth cheapest generic doxycycline uk, are the modes of presentation taking antibiotics for sinus infection while pregnant buy doxycycline 200 mg line. Diagnosis is by barium swallow virus 360 effective doxycycline 200mg, which identifies extrinsic compression of the esophagus in the region of the aortic arch. Management consists of surgical division of a portion of the constricting ring of vessels. The specific surgical plan must be tailored to the particular type of aortic arch anomaly present. Complete esophageal obstruction results in inability of the infant to handle his or her own secretions, producing "excess salivation" and aspiration of pharyngeal contents. After delivery, the infant typically is unable to swallow saliva, which drains from the corners of the mouth and requires frequent suctioning. Attempts at feeding will result in prompt regurgitation, coughing, choking, and cyanosis. Diagnosis is established by attempting to pass a nasogastric tube and meeting resistance at 10-12 cm from the nares followed by chest x-ray film for confirmation. Chest x-ray film will show the tube to end or coil in the region of the thoracic inlet. The x-ray film should also be examined for possible skeletal anomalies, pulmonary infiltrates, cardiac size and shape, and abdominal bowel gas patterns. Some surgeons perform preliminary gastrostomy to decompress the stomach and provide additional protection against reflux. Obstruction of the lumen of the duodenum may be either complete or partial, pre or postampullary, and caused by either intrinsic or extrinsic problems. Duodenal atresia results in complete obstruction of the lumen of the duodenum, whereas symptoms of partial obstruction result from a stenotic lesion. Annular pancreas is a congenital anomaly of pancreatic development, which results in an encircling "napkin ring" of pancreatic tissue about the descending duodenum. Malrotation may cause complete or partial duodenal obstruction in one of two ways. The entire midgut may twist on the pedicle of its blood supply, the superior mesenteric artery, resulting in duodenal obstruction and eventual nonviability of the midgut. The presence of Down syndrome, esophageal atresia, or imperforate anus suggests duodenal atresia. Midgut volvulus typically presents with symptoms of duodenal obstruction (bilious vomiting) and evidence of intestinal ischemia (mucoid bloody stools), usually in an infant who for days or weeks has eaten and stooled normally. Differential diagnosis includes duodenal atresia (stenosis), annular pancreas, and malrotation with or without the complication of midgut volvulus. The exact cause of the obstruction may not be known until a laparotomy is performed. In complete duodenal obstruction, the pathognomonic x-ray finding is a "double bubble. It is important to eliminate malrotation as a possibility because its complication, midgut volvulus, is a true surgical emergency. In cases of atresia or annular pancreas, gastric suction will control vomiting and allow "elective" surgical correction. Malrotation mandates immediate surgical intervention because the viability of the intestine from the duodenum to the transverse colon may be at risk from midgut volvulus. Jejunal obstruction typically results from atresia of that segment of the bowel, usually caused by a vascular accident in utero. Infants with jejunal obstruction usually have bilious vomiting associated with minimal abdominal distention, because few loops of intestine are involved in the obstructive process. A plain abdominal x-ray study reveals only a few dilated small bowel loops with no gas distally. Uncomplicated (simple) obstruction of the terminal ileum by pellets of inspissated meconium. Complicated meconium ileus, implying compromise of bowel viability either prenatally or postnatally. Infants with obstructing lesions in the distal intestine have similar signs and symptoms. They typically have distended abdomens, fail to pass meconium, and vomit bilious material. Abdominal x-ray studies show multiple dilated loops of intestine; the site of obstruction (distal small bowel vs colon) cannot be determined on plain x-ray films. The procedure can identify and treat meconium plug-hypoplastic left colon syndrome. A sweat test may be needed to document cystic fibrosis in cases of meconium ileus (unlikely to be helpful in the first few weeks of life). However, laparotomy is often necessary to determine the exact nature of the problem in infants with normal results of barium enema. Nonoperative management is "curative" in cases of meconium plug and hypoplastic left colon. Passage of time and colonic stimulation by digital examination and rectal enemas promote return of effective peristalsis. Interestingly, uncomplicated meconium ileus, if identified, can often be treated by nonoperative means. Repeated enemas with Hypaque or acetylcysteine (Mucomyst) may disimpact the inspissated meconium in the terminal ileum and relieve the obstruction. Surgical intervention is required for atresia of the ileum or colon, for complicated meconium ileus, and when the diagnosis is in doubt. Some surgeons are performing "one-stage" pull-through procedures, without preliminary colostomy. The rectum ends above the puborectalis sling, the main muscle responsible for maintaining fecal continence. In males, there may be a rectourinary fistula, and in females, a rectovaginal fistula. Variants include anal stenosis, imperforate anus with perineal fistula, and imperforate anus without fistula. All patients with imperforate anus should have x-ray studies of the lumbosacral spine and urinary tract because there is a high incidence of dysmorphism in these areas. Surgical therapy in the neonate consists of colostomy for high anomalies and perineal anoplasty or dilation of fistula for low lesions. If the level is not known, colostomy is preferable to blind exploration of the perineum. If colostomy is done, a contrast x-ray study of the distal limb should be performed to ascertain the level at which the rectum ends and to determine the presence or absence of an associated fistula. Choanal atresia is a congenital blockage of the posterior nares caused by persistence of a bony septum (90%) or a soft tissue membrane (10%). Unilateral or bilateral obstruction at the posterior nares may be secondary to soft tissue or bone. Choanal atresia, which is complete and bilateral, is one of the causes of respiratory distress immediately after delivery. The effects of upper airway obstruction are compounded because neonates are obligate nose-breathers and will not "think" to breathe through the mouth. Respiratory distress resulting from partial or total upper airway obstruction is the mode of presentation. Diagnosis is based on an inability to pass a catheter into the nasopharynx via either side of the nose. Simply making the infant cry and thereby breathe through the mouth will temporarily improve breathing. Insertion of an oral airway will maintain the ability to breathe until the atresia is surgically corrected. Airway obstruction is produced by posterior displacement of the tongue associated with the small size of the mandible. Severity of symptoms varies, but most infants manifest a high degree of partial upper airway obstruction. Infants with mild involvement can be cared for in the prone position and fed through a special Breck nipple. More severe cases require nasopharyngeal tubes or surgical procedures to hold the tongue in an anterior position.
However antibiotic resistance bacteria doxycycline 100 mg visa, the majority of studies do not include recommendations of what meaningful changes clinicians 16 should expect or aspire to infection red line purchase 100 mg doxycycline visa. The objectives of this systematic review are to locate reports on the clinical effectiveness of conservative lymphedema management by reporting on outcomes which use anchor-based and distribution-based approaches bacteria wanted poster doxycycline 200mg mastercard. The key words for the search were "lymphedema" or "lymphoedema" and "responsiveness" or "clinically significant" or "clinically important" or "measurement error" or "minimally clinical important change" or "minimal clinical change" or "small real difference antibiotics for recurrent urinary tract infections discount doxycycline 100 mg without a prescription. After title and abstract screening, 416 of 483 articles were excluded where there was no report on conservative interventions. Articles that used imaging procedures as an outcome were excluded, as well, since they are used more as research tools than clinical assessment tools. The remaining articles (n = 67) were stratified into the outcomes of interest: volume, symptoms, skin changes, infection rate, quality of life, strength, function, and disability. Then, 43 articles were excluded as non-relevant due to the use of the term "clinically important" without any discussion on clinically important definitions, outcomes, or recommendations (Figure 2. There are different tools for measuring volume: water displacement, volume derived from calculations of circumferential measurements, and perometry. Basic circumferential measurements measured by a flexible tape are the most commonly used in clinical practices. These studies are reported in this review according to reliability (8 studies), immediate change after an intervention (2 studies), changes after intensive phase (3 studies), and changes in maintenance phase (7 studies). Their results take into consideration the time factor that is important in lymphedema, since lymphedema tends to change over the hours of the day, and from day to day. Their results emphasize the need to use segmental volumes in decision-making, rather than the volume calculations of the whole arm. For those clinicians who do not calculate volume from the circumferential measurements, this study provides valuable clinical information with its estimation of what to expect using a flexible tape alone or when teaching patients self-measuring. In their study, they reported on an intra-observer variable that measures repeatability and an inter-observer variable that measures reproducibility. In this case, the changes in leg volume can be reliably defined when taken by several observers only when it exceeds 1,000ml and beyond 270ml when taken by one observer. A few studies have examined the immediate effect of interventions and discussed their meaningfulness. Both studies demonstrate a cut-off point beyond which a change will be considered. The authors reported effect sizes which were not different between interventions; however, they were clinically meaningful when compared to baseline. Although the changes demonstrated in these studies were large, the clinician will want to know whether, for example, a 50% reduction is sufficient for the patient to recognize improvement, or whether he/she will feels the difference between a 30% vs 40% change A comparison to an anchor-based method approach would have helped to answer these questions. Therefore, a meaningful change, for better or for worse, needs to be defined in order for clinicians to decide when to actively intervene. In this review, studies in which the intervention ended, but further reduction was expected as a long-term effect, were included, as well. This experience strengthens the decision that a 5% increase would be sufficient for intervention, since treatment delivery caused a decrease back to normal (Katz et al. They found that both groups did not change over 6 months; thus, adding electrical stimulation to the use of a sleeve showed no effect. Despite the lack of information on the expected changes in excess limb volume in the self-management phase, the authors who conducted this study found that a difference of 2. To determine whether this change is important to the patient will need further investigation with anchor-based approaches. There is inconsistency between studies as to what is considered a change in volume and, moreover, what is meaningful change. If stability is satisfactory, the patient can move into the next stage: the maintenance phase. Knowledge of what is considered to be a stable state and what is defined as deterioration can help the clinician advise correctly on how to maintain and when intervention might be necessary. However, these studies did not describe what is considered to be a clinical change (Belmonte et al. Their study examined aerobic exercise versus resistance exercise and found that the aerobic group reported less symptoms from baseline. They concluded that this was meaningful change (Buchan, Janda, Box, Schmitz, & Hayes, 2016). These outcomes can validate the results of treatment, especially where other objective variables, such as volume, do not respond to treatment. The oncologist palpated the participants and quantified the amount of induration by a scale (0=none, 1=a little, 2=quite a lot, 3= very much). The authors concluded that this definition should be clinically meaningful since an improvement of 2 grades could not be due to a measurement error. Additionally, the patients 26 were asked to describe how their arm felt at the end of the follow-up period. Eight of 15 (53%) patients had a moderate lessening of induration in the examined areas. These findings were supported by the fact that 63% (12 of 19) participants reported that their arms felt softer (Todd et al. This is an example of a study that provides a patient perspective in addition to the objective outcome. Infection rate was one of the parameters for stability (not more than one infection episode in the past 3 months) (Katz et al. This leaves clinicians with no recommendations as to what changes to expect that will be meaningful to the patient/health system (cost, for example) from the results of different questionnaires administered in clinical practice (Belmonte et al. Knowing what will be effective for patients in other aspects of their lives will enable clinicians to incorporate other modalities or therapies and consider cost-effectiveness, as well. Conclusions Lymphedema is a chronic condition which requires life-long management. As clinicians, deciding whether to change our practices, adopt new devices or techniques, invest in education, and refer to new therapies, we need to have more information than statistical significance alone. We need to know whether our patients will be happier, or healthier, with the available intervention. The purpose of this article was to review the clinical effectiveness of conservative lymphedema management outcomes by anchor-based and distribution based approaches. Some of the studies did use cut-off points, especially when describing an intervention used during the maintenance phase when patients should be stable and there is a concern for exacerbation (Schmitz, Ahmed, et al. The lymphedema population which is most researched is that of breast cancer survivors. Clinicians tend to generalize decision to their own patients based on the results of breast cancer studies. In this way, researchers and clinicians will be able to understand and explore the findings and to transfer this new knowledge to practice. For example, with volume as an outcome, the clinician will aim for "maximum" reduction until stabilization to order a garment; the patient will want "just enough" so he can bend his knee, climb stairs, etc. Effects of Complete Decongestive Therapy on the Incidence Rate of Hospitalization for the Management of Recurrent Cellulitis in Adults with Lymphedema. Efficacy of low-frequency low-intensity electrotherapy in the treatment of breast cancer-related lymphoedema: a cross-over randomized trial. Conservative treatment of postmastectomy lymphedema: a controlled, randomized trial. Erysipelas as a sign of subclinical primary lymphoedema: a prospective quantitative scintigraphic study of 40 patients with unilateral erysipelas of the leg. Journal of the American College of Surgeons, 206(5), 1038-1042; discussion 1042-1034. A Randomized Trial on the Effect of Exercise Mode on Breast Cancer-Related Lymphedema.
Unfortunately antimicrobial medication buy doxycycline 100 mg with amex, this pain killing activity antibiotic resistance natural selection order cheap doxycycline line, but prevent the agonists from causing is not necessarily true with respect to neuropathic pain antibiotic 6340 doxycycline 200 mg discount. Some opioids actually have Opioids are effective in neuropathic pain infection hacked buy doxycycline with a mastercard, but one has to use divergent actions at different receptors, being an agonist at much more of them than in other pain conditions. Opioids bind to several different receptors; these In summary, drugs affect nerves to stop the processes receptors normally bind to our own naturally produced of central and peripheral sensitization by binding to internal painkiller substances. Opioids are external agents receptors localized on various nerve membranes in that we administer. The binding of recently Duloxetine (Cymbalta), have been opioids to any of these receptors causes pain relief. These agents are associated with many less side cause the untoward side effects that are sometimes effects than the tricyclic agents. Most of its pain killing effects via another mechanism besides descending modulation (about 70%) come from modulation of norepinephrine to directly prevent/reduce central sensitization. Methadone is a good example of a drug the treatment/prevention of central sensitization. Methadone acts to From the media, you may be aware of Gabapentin disrupt central sensitization. The great breakthrough with respect to chosen for the treatment of neuropathic pain, Gabapentin is that it was not more efficacious than methadone makes a good choice. Most side the antidepressants exist in old (tricyclic) and effects associated with Gabapentin are dizziness and newer forms (serotonin-specific reuptake inhibitors). More recently, a new agent, Pregabalin Antidepressants work by preventing the release of (Lyrica), has become available. Pregabalin works in chemicals such as norepinephrine and serotonin exactly the same manner as Neurontin. In essence, they block the reuptake In the studies that have been done, Pregabalin has of norepinephrine and serotonin after they are released about the same side effect profile as Gabapentin. The older agents are referred to as tricyclic Pregabalin may cause some degree of euphoria. An exciting new development in the treatment of these agents are associated with many side effects such neuropathic pain is the use of botulinum toxin type A as: dry mouth, constipation, sedation and sleepiness, (Botox). Newer agents specifically only affect bacterium Clostridium botulinum and is a true the re-absorption of serotonin into nerves. Botox was at first released for the treatment of insertion of a temporary catheter into the spine and painful hypertrophic muscular conditions such as cervical administration of the drug being considered for use. In such conditions, it binds to certain nerve patient obtains pain relief without side effects, he/she is a terminals and prevents the release of chemicals. Unlike with spinal acetylcholine) that would cause muscular spasm and cord stimulation, the patient is not in control of the pump contraction. However, botulinum toxin has been shown to and cannot affect how drugs are delivered. The physician work by inhibition of central sensitization in neuropathic sets the rate of drug delivery. There will be more news forthcoming regarding the patient must return to the physician at periodic intervals the potential uses of Botox. Spinal cord stimulation involves placement of leads We have then attempted to show how various medications (electrical wires) into the epidural space (the same space that and procedures can be utilized to treat pain via a mechanistic women receive local anesthetics to prevent labor pain). Spinal cord stimulation works by preventing transmission of electrical stimulation i. If the trial is successful, leads may be reinserted and Rosenstock J, Tuchman M, LaMoreaux L, Sharma U. Pregabalin for the treatment of painful diabetic periphertal neuropathy: a double-blind, placebo-controlled trial. Pain, 110(3): 628 buried under the skin and connected to a battery that is also 38, 2004 implanted under the skin. Lange Medical the stimulation feels by adjusting a hand-held programmer Books/McGraw Hill. Many different drugs (but usually opioids) can be administered through the pump by continuous infusion. Like spinal cord stimulation, a trial is first performed to see if the patient obtains pain relief. Adhesions: Tissue surfaces that are adherent or attached to each other, either loosely or firmly, as a result of wound healing and sometimes inflammation. Arachnoid: Delicate, web-like middle layer of the three membrane layers that cover the brain and spinal cord; arachnoid mater. Ascending tracts: Groups of nerve fibers in the spinal cord that transmit sensory impulses upward to the brain. Aseptic meningitis: Inflammation of the membranes (meninges) that cover the brain and spinal cord. Astrocytes: A type of neuroglial cell that functions to connect neurons to blood vessels. Ataxia: Impaired ability to coordinate the muscles in voluntary muscular movements; symptomatic of any of several disorders of the nervous system. Atrophy: A wasting of tissues or decrease in size of a part of the body because of disease or other influences. Autonomic nervous system: Portion of the nervous system that functions to control the actions of the visceral organs and skin; its actions are not under voluntary control. Barium swallow: An x-ray using barium to view the act of swallowing, the esophagus or stomach. Basal ganglion: Mass of gray matter located deep within a cerebral hemisphere of the brain; has important functions in automatic movements of the limbs and in the control of muscle tonus. Basilar impression: Upward displacement, particularly of the uppermost part of the cervical spine, into the region of the posterior fossa often producing compression of the brainstem and portions of the cerebellum. A patient with equal strength bilaterally means there is equal strength on both sides of the body. Brainstem: the portion of the brain that includes the midbrain, pons and medulla, thalamus and hypothalamus. Calamus sciptorius: Inferior part of the rhomboid fossa; the pointed lower end of the fourth ventricle of the brain. Canalization neurulation: the formation of canals or passages to form the neural tube during the early stages of embryonic development. Catheter: A tube designed for insertion into vessels, canals, passageways or body cavities to permit the injection or withdrawal of fluids or substances. Central canal: the opening or channel normally present through the length of the spinal cord in later fetal life and early infancy. It gradually disappears throughout childhood, but segments of it may remain in adults (see also hydromyelia). Central nervous system: the part of the nervous system consisting of the brain and spinal cord, which coordinates the entire nervous system of the body. Cerebellar speech: Abnormal speech patterns seen in people who have a disease of the cerebellum or its connections; a slow, jerky and slurred speech that may come and go or it may be unvaried in pitch. Cerebellum: Portion of the brain that lies in the posterior fossa and coordinates skeletal muscle movement. Cerebral aqueduct: A narrow conduit or passage between the third and fourth ventricles located in the midbrain. Cerebral hemisphere: One of the large paired structures that together constitute the cerebrum of the brain. Cerebral spinal fluid: Fluid occupying the ventricles of the brain, subarachnoid space of the meninges, and the central canal of the spinal cord. Cerebrum: Portion of the brain that occupies the upper part of the cranial cavity. Cervical: the area of the neck made up of seven cervical vertebrae, which are counted from top to bottom.
Additional information: