
Thomas Nguyen, MD
- Department of Emergency Medicine
- Beth Israel Medical Center, Albert Einstein College of Medicine
- New York, New York
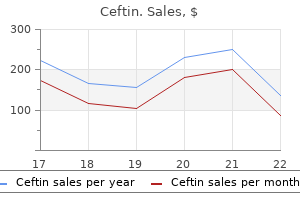
Persons using assistive technology may not be able to fully access information in this report antibiotics for acne birth control buy 500mg ceftin free shipping. None of the investigators have any affiliations or financial involvement that conflicts with the material presented in this report antibiotics in food discount ceftin 250 mg on line. Suggested citation: Skelly A bacteria zombie plants cheap ceftin 250 mg on-line, Hashimoto R antibiotic 24 hours not contagious order ceftin 500 mg line, Al-Khatib S, Sanders-Schmidler G, Fu R, Brodt E, McDonagh M. Key Informants are not involved in the analysis of the evidence or the writing of the report. Therefore, in the end, study questions, design, methodological approaches, and/or conclusions do not necessarily represent the views of individual Key Informants. Key Informants must disclose any financial conflicts of interest greater than $10,000 and any other relevant business or professional conflicts of interest. Because of their role as end-users, individuals with potential conflicts may be retained. Director, Cardiac Rapid Evaluation Unit Future of Family Medicine Professor Washington University Vice Chair, Department of Family and St. However, the conclusions and synthesis of the scientific literature presented in this report does not necessarily represent the views of individual reviewers. Peer Reviewers must disclose any financial conflicts of interest greater than $10,000 and any other relevant business or professional conflicts of interest. Because of their unique clinical or content expertise, individuals with potential nonfinancial conflicts may be retained. The quality of included studies was assessed, data were extracted, results were summarized qualitatively and using meta-analysis, and the strength of the evidence was graded for each primary outcome. There was insufficient evidence to draw conclusions for all other long-term primary outcomes including stroke, myocardial infarction, and congestive heart failure. Firm conclusions regarding health-related quality of life were not possible given heterogeneity across studies for instruments employed, measurement timing, and clinical characteristics. Exercise capacity and related outcomes from randomized controlled trials comparing radiofrequency ablation with medical therapy. Atrial fibrillation is characterized by uncoordinated atrial activation with resulting 4, 5 deterioration of atrial mechanical function. Typically, pharmacologic therapy is the primary treatment for rate and rhythm control, while pulmonary vein isolation with catheter ablation is reserved for second-line treatment but may be appropriate 5 as a first-line treatment in select populations when a rhythm control strategy is desired. Rhythm control should not be used to allow patients to come off anticoagulation as the decision regarding anticoagulation 5 should be based on their risks of thromboembolic events and bleeding. Selection of the first-line antiarrhythmic medication is largely driven by the presence or absence of structural heart disease. In patients with heart failure, the guidelines recommend one of two antiarrhythmic medications as 5 first-line therapy (dofetilide and amiodarone). Side effects can occur with the use of antiarrhythmic medications; some may actually cause more arrhythmias and some may lose effectiveness over time. Patients on these medications therefore need to be monitored to assess the impact of medications on heart rhythm and the potential for side effects and interactions with any concomitant medications such as anticoagulants. Relief of symptoms is a primary reason for considering catheter ablation as a treatment strategy. For the procedure to be successful, complete bi- directional electrical isolation of all pulmonary veins should be achieved. Recent systematic reviews attempted to 23-25 evaluate the efficacy of approaches relative to each other, but significant heterogeneity with 23 regard to the approaches compared precluded meaningful conclusions. The comparative effectiveness and harms of catheter ablation in the Medicare population (65 years of age or <65 years of age and permanently disabled) were not explored. The 2009 report did not compare cryoablation with medical therapy or compare catheter ablation energy sources with one another. Procedural volume was associated with probability of in-hospital death but not with overall risk of complications. An almost two-fold increase in the number of patients treated with catheter ablation was reported between 2003 and 2006 compared with the number treated between 1995 and 2002 based on a world-wide survey of electrophysiology 27 centers. Anecdotally, utilization has continued to increase in the Medicare and general populations. For purposes of this report, efficacy refers to the ability of a treatment to produce a desired effect under optimum controlled conditions, such as during a randomized controlled trial. Effectiveness refers to the effect of treatment in actual clinical practice as evaluated by observational studies or comparative pragmatic trials. The analytic framework (Figure A) shows the target population, interventions and outcomes that were examined. Comparisons of interest include: a) Catheter ablation compared with medical therapy b) Comparing ablation using different energy sources Key Question 2. Analytic framework for catheter ablation for atrial fibrillation *Patients with longstanding persistent atrial fibrillation, persistent atrial fibrillation, or paroxysmal atrial fibrillation (considered separately); includes general population and Medicare population. The Key Informant panel included experts in cardiology primarily (with specialties in electrophysiology, heart failure, and cardiovascular aging/cardiovascular disease in older adults) and internal medicine; representatives from relevant specialty societies; government representatives. Key Informant input during topic refinement confirmed that this was a logical approach. Reference lists of included articles and relevant review articles were inspected for relevant publications. All citations were reviewed independently by two individuals at both the title/abstract and full-text level and differences were resolved by consensus. For all Key Questions, the focus was on evidence from comparative studies with the least potential for bias. Comparative observational studies were required to have a minimum of 100 patients to be included. Registry and administrative data studies were considered if inclusion criteria were met. For Key Question 2, case series that were specifically designed to evaluate harms and/or adverse events following ablation, had a minimum of 1000 patients and at least 80 percent followup were included because all included comparative studies were relatively small in size. For all Key Questions, both long-term (>12 months) and short-term (12 months) outcomes were reported. The primary outcomes (see Rating the Body of Evidence below) were considered to be the most clinically important and were the focus of reporting, decisions for data pooling and determination of overall strength of evidence. Where applicable and where data were available, results from short-term (12 months) and long-term (>12 months) followup were described. Each full-text article was independently evaluated for final inclusion by two investigators. After data extraction, at least one other staff member and one study investigator each verified the accuracy and completeness of abstraction for each study included. Comparative observational studies were assessed for study design features and sources of potential bias. Two investigators independently assessed the quality of each study, and any discrepancies were resolved through discussion and consensus. Studies rated good are considered to have the least risk of bias and their results are considered valid. Studies rated fair are susceptible to some bias, though not enough to invalidate the results. The study may be missing information, making it difficult to assess limitations and potential problems. The fair-quality category is broad, and studies with this rating will vary in their strengths and weaknesses. They have a serious or fatal flaw in design, analysis, or reporting; large amounts of missing information; discrepancies in reporting; or serious problems in the delivery of the intervention. The results of these studies are least as likely to reflect flaws in the study design as the true difference between the compared interventions. Studies rated as being poor in quality a priori were not excluded, but considered to be less reliable than higher-quality studies when synthesizing the evidence, particularly if discrepancies between studies are present. Data Synthesis Meta-analysis was conducted in order to provide more precise estimates for outcomes when adequate data were reported. To determine the appropriateness of meta-analysis, clinical and methodological diversity and assessed statistical heterogeneity were considered.
Categories Parietal include daily bacterial folliculitis buy generic ceftin 250mg line, persistent antibiotic resistant infections 500 mg ceftin with mastercard, rare or none antibiotics zone of inhibition chart buy ceftin cheap, undefined antibiotic resistance studies safe 250mg ceftin, and Occipital unknown (Table 18. Anterior border to the frontal lobe is the precentral sulcus; inferior border to the temporal lobe is the sylvian fissure (14). Advantages of the Five-Dimensional bOther locations, such as subcortical regions (e. The classification process is independent of the amount of Seizures frequently consist of more than one clinical compo- available diagnostic information (medical history, electroen- nent and follow a certain time sequence (e. The more information is available, the ening and generalized rhythmic jerking of the body). A syndromic term can semiologic detail, up to four seizure phases can be separately be added when the case represents a typical syndromic manifes- classified. This restriction is arbitrary but usually sufficient to tation and use of the syndromic name can convey more informa- classify all the important seizure components based on clinical tion with fewer words. Important variations in clinical presenta- experience with this system in the past two decades. A persistent pattern must be recogniz- able in the period before the past 6 months. This process includes a continu- ous refinement of the seizure semiology, epileptogenic zone, Other and etiology as more information (e. Commission on Classification and Terminology of the International Repeated epileptic seizures are the presenting symptoms of local- League Against Epilepsy. History of epilepsy and seizure classifica- seizure as an independent neurologic symptom due to multiple tion. Commission on Epidemiology and Prognosis, International League Against quencies and in conjunction with other clinical findings. Classifications of the International League Against Epilepsy: time for reappraisal. A proposal for a five- therefore more surgically oriented and neglects subtypes of dimensional patient-oriented epilepsy classification. Reply to Of Cabbages and kings: some con- siderations on classifications, diagnostic schemes, semiology, and con- Concept of the Epileptogenic Zone cepts. A population-based survey of childhood epilepsy in Okayama Prefecture, Japan: reclassification by a the multifactorial approach to epilepsy, it always remains a newly proposed diagnostic scheme of epilepsies in 2001. Specific epileptic syn- dromes are rare even in tertiary epilepsy centers: a patient-oriented and the available tests. The syndromic classification of the International League Despite attempts to base the etiologic dimension on an iso- Against Epilepsy applied to epilepsy in a general population. The syndromic classification of the or anatomy, we were not able to describe epilepsy etiology at International League Against Epilepsy: a hospital-based study from South only one level. Comparison of classifications of the classification of epilepsies is currently controversial, with seizures: a preliminary study with 28 participants and 48 seizures. Application of semiological seizure classifi- attempt to improve its limitations, with the ultimate goal of cation to epileptic seizures in children. Proposal for revised classification of epilepsies tion of seizures to provide localization information. International League Against Epilepsy (1989) Seizures occur in clusters at intervals or randomly. Complex partial seizures often but not always beginning At present, the following syndromes are established, but with motor arrest typically followed by oroalimentary more may be identified in the future: automatism. Temporal spikes, sharp waves and/or slow waves, unilat- which are based mainly on seizure types and other clinical fea- eral or bilateral, synchronous but also asynchronous. Inferences regarding anatomic localization may allow better definition of the intracranial distribu- must be drawn carefully. Seizure symptomatol- (a) a unilateral or bilateral interruption of background activity ogy and, sometimes, additional clinical features often provide and (b) temporal or multilobar low-amplitude fast activity, important clues. The first sign or symptom of a seizure is often rhythmic spikes, or rhythmic slow waves. Intracranial recordings may provide additional reflect its further propagation through the brain. This information regarding the chronologic and spatial evolution sequence, however, can still be of high localizing importance. One must bear in mind that a seizure may start in a clinically silent region, so that the first clinical event occurs only after Amygdalo-Hippocampal (Mesiobasal Limbic spread to a site more or less distant from the locus of initial or Rhinencephalic) Seizures discharge. The following tentative descriptions of syndromes Hippocampal seizures are the most common form; the symp- related to anatomic localizations are based on data which toms are those described in the previous paragraphs except include findings in studies with depth electrodes. Seizures are characterized by rising epigastric discom- seizures, complex partial seizures, and secondarily generalized fort, nausea, marked autonomic signs, and other symptoms, seizures, or combinations of these. Frequently, there is a his- tory of febrile seizures, and a family history of seizures is com- 1 Reproduced, with permission, from Commission on Classification mon. On metabolic imaging stud- and Terminology of the International League Against Epilepsy. Proposal for revised classification of epilepsies and epileptic syn- Unilateral or bilateral temporal lobe spikes are common on dromes. Simple partial Lateral Temporal Seizures seizures, particularly partial clonic facial seizures, are com- Simple seizures characterized by auditory hallucinations or illu- mon and may be ipsilateral. If secondary sensory changes sions or dreamy states, visual misperceptions, or language disor- occur, numbness may be a symptom, particularly in the hands. Motor cortex epilepsies are mainly characterized by simple partial seizures, and their localization depends on the side and topography of the area involved. In cases of the lower pre- Frontal Lobe Epilepsies rolandic area, there may be speech arrest, vocalization or dys- phasia, tonic-clonic movements of the face on the contralateral Frontal lobe epilepsies are characterized by simple partial, side, or swallowing. Generalization of the seizure frequently complex partial, secondarily generalized seizures, or combina- occurs. Seizures often occur several times a day and fre- march or Jacksonian seizures occur, particularly beginning in quently occur during sleep. Status epilepti- involving the paracentral lobule, tonic movements of the ipsi- cus is a frequent complication. Features strongly suggestive of the diagnosis include the Kojewnikows Syndrome following: Two types of Kojewnikow syndrome are recognized, one of 1. Complex partial seizures arising from the frontal lobe, among the epileptic syndromes of childhood noted under symp- often with minimal or no postictal confusion. Rapid secondary generalization (more common in rolandic partial epilepsy in both adults and children and is seizures of frontal than of temporal lobe epilepsy). Such epilepsies include those with pre- and postcentral sympto- Cingulate matology (perirolandic seizures). Such overlap to adjacent Cingulate seizure patterns are complex partial with complex anatomic regions also occurs in opercular epilepsy. Autonomic signs are In frontal lobe epilepsies, the interictal scalp recordings common, as are changes in mood and affect. Intracranial recordings can sometimes dis- or initial loss of contact and adversive movements of head and tinguish unilateral from bilateral involvement.
The pathology of atopic dermatitis is a chronic inammation of the skin that is aggravated by the deterioration of compliance bacteria 33 000 feet order 500 mg ceftin visa. Environmental factors necessary to educate patients repeatedly so they may understand Allergens such as mites and house dust treatment for recurrent uti by e.coli buy 500 mg ceftin overnight delivery, pollen allergens in the pathology and realize that a long-term antiinammatory specic seasons virustotalcom cheap 500mg ceftin with mastercard, and organic solvents such as formaldehyde and therapy is required human eye antibiotics for dogs discount generic ceftin canada. Being sensitized to mites in in- fancy is reportedly a marker for the development of asthma. Summary of the basic therapy of atopic dermatitis Periocular pathological changes are often observed during air- 6. These are If no infectious symptoms are seen in the affected part, a topical investigation and countermeasures of causes and exacerbating steroid can be applied to encourage the improvement of the cuta- factors; second, correction of skin dysfunctions (skin care); and neous symptom, even if the site is densely populated with Staph- third, pharmacotherapy. These are based on the concept that this ylococcus aureus (with bacterial counts of 1000 cfu/10 cm2 or more disease is an inammatory cutaneous disease that forms an as detected by the stamp method). These 3 points are equally (2) Care should be taken against microbial substitution with important and thus need to be appropriately combined in accor- methicillin-resistant S. Contact antigen skin barrier functions of patients with atopic dermatitis are Contact dermatitis is divided into allergic contact dermatitis, deteriorated due to abnormality in function such as deteri- which is developed by a sensitized patient, and primary irritant orated water retentivity, lowered threshold of itch, and contact dermatitis, which can be developed by anyone depending susceptibility to infection. Stress (3) Basics of pharmacotherapy: If countermeasures against the Aggravation by mental stress is often experienced in daily causes and exacerbating factors and the skin care have not medical practice. The high rate of aggravation of atopic dermatitis resulted in improvement of dermatitis, pharmacotherapy reported in areas affected by the Great Hanshin-Awaji Earthquake will be needed. Scratching will not only damage the cutaneous barrier functions b) Assessment of severity and activity level: Attempts have by injuring the skin, but also worsen the symptoms by causing the been made to assess the severity and activity level by release of various phlogogenic agents. If no improvement is observed or if an abnormal medication, such oral administration may be used for a change in symptoms is observed after approximately 1 short period of time. If remission cannot be main- If an abnormal change is observed in symptoms during treat- tained after approximately 6 months, the patient should ment or if no improvement is observed after treatment based on a be referred to a specialized medical institution to dene basic therapy for approximately one month, referral to a more the condition as severe, most severe, or intractable, in specialized medical institution should be considered. Skin care against atopic dermatitis execute): If remission cannot be maintained, external Skin care is highly important, as is shown by consideration of application of a higher ranked steroid, oral administration the fact that the skin tends to become more prone to drying due to of immunosuppressive agents (cyclosporine), oral aging, and given the adverse effects of settlement of S. In such conditions, with facilitation of transcutaneous invasion of Oral administration of steroids should not be executed in allergens and irritants, likely resulting in allergic reactions and ir- principle. However, if the patient develops extremely ritability, patients may come to suffer from itch due to the lowered 238 I. Abnormality in the water barrier function and the water retention capability of the horny cell layer are considered as causing/exacerbating factors of atopic dermatitis. Accordingly, the incidence rate of atopic dermatitis could be decreased by mois- turizer application during the newborn period. If the bacterial count is larger, it is important to take a skin care regimen with consideration of the bacterial ora on the skin surface. Given that a moisturizer is known to exert a higher moisturizing effect when externally applied twice a day than when applied once a day, consid- eration should be given to the number of external applications. Therefore, physicians should instruct patients not to forget the external application of 8. In the sweaty summer season, mild cases with the aim of moistening and protecting the skin, washing away sweat by showering improves rashes. For the treatment of weeping lesions in the such regions as the hairline, the side of the nose, and jaws, acute phase, a surface dressing with a zinc ointment may be etc. Urea preparations should be used with caution, as they can stimulate an eroded surface or strongly inammatory skin. Pharmacotherapies for atopic dermatitis turizer is useful to prevent relapse of atopic dermatitis; however, 8. External medicine studies have shown that the continuous use of a moisturizer since 8. Topical therapy the newborn period may reduce the incidence rate or delay the Topical therapy refers to skin care chiey with moisturizers, and development of atopic dermatitis. There ointment or topical steroids intermittently in combination with a they activate steroid-responsive genes to exert their pharmaco- moisturizer is useful in the remission maintenance period. This logical actions that include antiinammatory action in a narrow therapy is referred to as proactive therapy (Fig. Administration method of topical steroids not only control the relapse of cutaneous symptoms, but also to be (1) Selection of topical steroid: Topical steroids are classied into cost-effective. A steroid of an appropriate Health Care, Nara, Japan) with an externally applied medicine is rank should be used in accordance with the severity of effective for the prevention of scratching. A dose for children is also in consideration of progressive reduction, intermittent proposed. Acne-like rash, including folliculitis and rosacea steroid to identify any side effects and the need for 2. Epidermal-dermal atrophy, dermal vulnerability (most likely to occur on the stepping down or stepping up the dose. The absorption geriatric or sunlight damaged skin, intertriginous zone, or facial surface) ratio of steroids varies signicantly among skin sites. Hidden or exacerbated dermatophyte infection limus ointment while gradually stepping down the dose. Contact dermatitis c) Monitoring of the dose of topical steroid: Monitoring (i) May be caused by an ingredient of the preservative or other base material. Improvement in symptoms should be react with a corticosteroid molecule of similar structure. Topical immunosuppressant (tacrolimus ointment class or higher shows no difference in efcacy after 3 [Protopic ]) weeks or more between twice-a-day external applica- (1) Pharmaceutical form and mechanism of action of tacrolimus tion and once-a-day external application. It is recom- ointments: Tacrolimus ointments will be used when existing mended that a strong topical steroid be initially applied therapies are not effective enough or not indicated because twice a day and then changed to once-a-day application of side effects. It should be used in consideration of pre- after remission of an acute or intractable lesion is cautions and after obtaining informed consent from the observed, for the purpose of enhancing the compliance patients. The action mechanism of advised against discontinuing the use of the drug on his tacrolimus is the inhibition of the function of T lymphocytes, own judgment. In addition, sufcient explanation should which play a central role in the development of allergic be provided to the patient about the side effects likely to inammation, and improvement in the barrier function. This property is considered an advantage tion) was reported mostly on the face and genital area because they are more absorptive and effective for the (99. Excessive exposure to ultraviolet light should be a topical steroid should be administered at a necessary avoided when the ointment is applied externally. If systemic aggravation is observed, tacrolimus ointment for adults should be administered at a the patient should be hospitalized for a short period and a dose of 5 g or less. The tacrolimus ointment should be administered at a methods for children are divided intothe age groups of <2 maximum of twice per day. When applied twice per day, an years of age, 2e12 years of age, and >13 years of age. Care interval of approximately 12 h between applications is rec- should be taken so that insufcient administration for ommended. Occlusive dressing therapy should not be used fear of side effects likely generated in the treatment of because it may cause an increase in the blood level. It is reported that twice-a-day external adverse events were observed in a study of post-marketing application of a moisturizer (preparation containing hep- prolonged administration; therefore, tacrolimus ointments arinoid) signicantly inhibits the relapse of inammation of are considered safe. Precautions for the use of tacrolimus atopic dermatitis compared with the untreated group (no ointment include the possibility of skin effects such as a application group). This problem can be managed by using a mois- (3) Side effects turizer before the application of the ointment or by using a a) Central nervous system effect: the drug generally gener- tacrolimus ointment in combinationwith a topical steroid for ates side effects in the form of sleepiness, loss of con- a short period of time. Combinations with other external centration, or malaise, and it may cause excitement if medicines should be avoided because of potential effects on administered in a large quantity. Precaution is necessary the stability and absorptive properties of the tacrolimus in use of antihistaminics in children, particularly against ointment. A second-generation antihistaminics is char- rashes associated with infectious diseases of the skin. In addition, cause dry mouth, sense of mucosal dryness, urinary tacrolimus ointments cannot be applied for reasons of safety retention, and so on. This drug is contraindicated for pa- to patients with nephropathy, pregnant women, infants tients with glaucoma or lower urinary tract obstructive younger than 2 years of age (at this point in time), and pa- disease (prostatomegaly, etc. Regarding the risk of lym- c) Digestive symptoms: these include nausea, vomiting, phoma and skin cancer, it has been reported that the external diarrhea, and abdominal pain.
Eligible patients enrolled into this study had previous inadequate response to topical medication antibiotics sinus infection npr purchase cheap ceftin on line. Patients received 1) an initial dose of 400 mg dupilumab (two 200 mg injections) on day 1 2012 antimicrobial susceptibility testing standards buy ceftin, followed by 200 mg once every other week (Q2W) for patients with baseline weight of <60 kg or an initial dose of 600 mg dupilumab (two 300 mg injections) on day 1 antibiotics for dogs how long discount 250mg ceftin, followed by 300 mg Q2W for patients with baseline weight of 60 kg; 2) an initial dose of 600 mg dupilumab (two 300 mg injections) on day 1 antibiotic resistance coalition buy ceftin 500mg line, followed by 300 mg every 4 weeks (Q4W) regardless of baseline body weight; or 3) matching placebo. Clinical Response the efficacy results at week 16 for adolescent atopic dermatitis study are presented in Table 11. Efficacy data from this study suggests that clinical benefit provided at week 16 was sustained through week 52. Patients were enrolled without requiring a minimum baseline blood eosinophil or other type 2 inflammatory biomarker (e. Annualized rate of severe asthma exacerbation events during the 24-week placebo controlled treatment period was also determined. Results were evaluated in the overall population (unrestricted by minimum baseline eosinophils or other type 2 inflammatory biomarkers) and subgroups based on baseline blood eosinophils count. Patients were randomised to receive either 200 mg (N=631) or 300 mg (N=633) Dupixent every other week (or matching placebo for either 200 mg (N = 317) or 300 mg (N= 321) every other week) following an initial dose of 400 mg, 600 mg or placebo respectively. The primary endpoint was the percent reduction in oral corticosteroid dose assessed in the overall population, based on a comparison of the oral corticosteroid dose at weeks 20 to 24 that maintained asthma control with the previously optimized (at baseline) oral corticosteroid dose. The demographics and baseline characteristics of these 3 studies are provided in Table 12 below. All patients were on oral corticosteroids for at least 6 months prior to the study initiation. In this 24-week trial, asthma exacerbations (defined as a temporary increase in oral corticosteroid dose for at least 3 days) were reduced by 59% in subjects receiving dupilumab compared with those receiving placebo (annualized rate 0. Effects on lung function, on oral steroid and exacerbation reduction were similar irrespective of baseline levels of type 2 inflammatory biomarkers (e. Rescue with systemic corticosteroids or surgery was allowed during the studies at the investigators discretion. Nasal congestion was rated daily by the subjects on a 0 to 3 categorical severity scale (0=no symptoms; 1=mild symptoms; 2=moderate symptoms; 3=severe symptoms). The demographics and baseline characteristics of these 2 studies are provided in Table 19 below. In the post-treatment period when patients were off dupilumab, the treatment effect diminished over time (see Figure 7a). The mean individual annualised prescribed total dose of systemic corticosteroids (in mg) during the treatment period was 71% lower in the pooled dupilumab group compared with the pooled placebo group (60. Efficacy with respect to severe asthma exacerbations and lung function was observed in both adolescents and adults. For the 200 mg every other week dose, patients had a reduction in the rate of severe exacerbations that was consistent with adults. Safety and efficacy in paediatric patients (< 12 years of age) with severe asthma have not been established. The European Medicines Agency has deferred the obligation to submit the results of studies with dupilumab in one or more subset of the paediatric population in atopic dermatitis and asthma (see section 4. The European Medicines Agency has waived the obligation to submit the results of studies with dupilumab in all subsets of the paediatric population in the treatment of nasal polyposis (see section 4. Steady-state concentrations were achieved by week 16 following the administration of 600 mg starting dose and 300 mg dose every other week or 300 mg dose every other week without a loading dose. Biotransformation Specific metabolism studies were not conducted because dupilumab is a protein. Elimination 34 Dupilumab elimination is mediated by parallel linear and nonlinear pathways. Elderly Of the 1,472 patients with atopic dermatitis exposed to dupilumab in a phase 2 dose-ranging study or phase 3 placebo-controlled studies, a total of 67 were 65 years or older. However, there were only 61 patients over 65 years of age included in this analysis. Of the 1,977 patients with asthma exposed to dupilumab, a total of 240 patients were 65 years or older and 39 patients were 75 years or older. Hepatic impairment Dupilumab, as a monoclonal antibody, is not expected to undergo significant hepatic elimination. Renal impairment Dupilumab, as a monoclonal antibody, is not expected to undergo significant renal elimination. No clinical studies have been conducted to evaluate the effect of renal impairment on the pharmacokinetics of dupilumab. Body Weight Dupilumab trough concentrations were lower in subjects with higher body weight with no meaningful impact on efficacy. No age-related pharmacokinetic difference was observed in adolescent patients after correction for body weight. If the carton needs to be removed permanently from refrigerator, the date of removal may be recorded on the outer carton. After use, place the pre-filled syringe or the pre-filled pen into a puncture-resistant container and discard as required by local regulations. Dupilumab 200 mg solution for injection in pre-filled pen Each single-use pre-filled pen contains 200 mg of dupilumab in 1. Table 1: Dose of dupilumab for subcutaneous administration in adolescent patients 12 years to 17 years of age with atopic dermatitis Body Weight of Initial Dose Subsequent Doses Patient (every other week) less than 60 kg 400 mg (two 200 mg injections) 200 mg 60 kg or more 600 mg (two 300 mg injections) 300 mg Adults the recommended dose of dupilumab for adult patients is an initial dose of 600 mg (two 300 mg injections), followed by 300 mg given every other week administered as subcutaneous injection. Consideration should be given to discontinuing treatment in patients who have shown no response after 16 weeks of treatment for atopic dermatitis. Some patients with initial partial response may subsequently improve with continued treatment beyond 16 weeks. If dupilumab treatment interruption becomes necessary, patients can still be successfully re-treated. Very limited data are available in patients with severe renal impairment (see section 5. Hepatic impairment No data are available in patients with hepatic impairment (see section 5. Body weight No dose adjustment for body weight is recommended for patients with asthma 12 years of age and older or in adults with atopic dermatitis (see section 5. For patients 12 to 17 years of age with atopic dermatitis, the recommended every other week dose is 200 mg (<60 kg) or 300 mg (60 kg). Paediatric patients the safety and efficacy of dupilumab in children with atopic dermatitis below the age of 12 years have not been established (see section 5. Method of administration Subcutaneous use Dupilumab is administered by subcutaneous injection into the thigh or abdomen, except for the 5 cm around the navel. For the initial 400 mg dose, two 200 mg injections should be administered consecutively in different injection sites. Reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy. This should be taken into consideration to determine type 2 status in patients taking oral corticosteroids (see section 5. Very rare cases of serum sickness/serum sickness-like reactions have been reported in the atopic dermatitis development program following the administration of dupilumab. Eosinophilic conditions Cases of eosinophilic pneumonia and cases of vasculitis consistent with eosinophilic granulomatosis with polyangiitis have been reported with dupilumab in adult patients who participated in the asthma development program. Patients with pre-existing helminth infections should be treated before initiating dupilumab. Conjunctivitis related events Patients treated with dupilumab who develop conjunctivitis that does not resolve following standard treatment should undergo ophthalmological examination (section 4.
Best buy for ceftin. Vital Signs: Staph infections can kill.