
Cynthia L. Rapp, BS, RDMS, RDCS
- Vice President of Clinical Program Development
- The Medipattern Corporation
- Toronto, Ontario, Canada
Stimulation of nerves in exercising muscles in turn leads to stimulation of the sympathetic nervous system type 2 diabetes medications uk 25 mg precose with mastercard. Sympathetic nerves cause the heart to beat faster diabetes type 2 brochure order 25mg precose otc, producing an increase in heart rate regulating diabetes in dogs order precose 50 mg free shipping. Air that is breathed into the lungs contains several kinds of gas metabolic disease doctors in nj discount 50 mg precose amex, including oxygen and carbon dioxide. In the lungs a lot of the oxygen travels into tiny blood vessels and binds to red blood cells. The oxygen is then used in chemical reactions with fuel sources such as fat or carbohydrate. These chemical reactions produce energy, and produce carbon dioxide as a waste product. It is possible to accurately measure how much carbon dioxide and oxygen is breathed in and out. This can be used to calculate how much has been used for the chemical reactions in the muscles. In McArdle people, this level of exercise causes a high heart rate and a high level of perceived exhaustion (it feels like really hard work to pedal) until 8-10 minutes into the exercise, when the second wind occurs (Abramsky, 2001). Many studies report that the amount of oxygen used is reduced in McArdle people compared to unaffected people. The authors suggest that McArdle people may use more oxygen because more oxygen is needed to produce energy from the breakdown of fats than the amount of oxygen needed to breakdown carbohydrates. A sugary drink (sucrose dissolved in water) would be quickly digested (broken down into glucose and fructose) and absorbed into the bloodstream. The glucose could then be used by the muscle cells to produce pyruvate by the process of glycolysis, and this pyruvate could then be used to produce energy. Having a sugary drink a couple of minutes before exercise seems to put the glucose into the bloodstream faster than the liver is able to . In the liver, glycogen which is stored in the liver must be converted to glucose (by liver glycogen phosphorylase), before the glucose can be released into the bloodstream. Having a sugary drink (or a glucose infusion given intravenously) will lead to a very high level of glucose in the blood. They found that a glucose infusion cause raised glucose levels (hyperglycaemia) and raised insulin levels (hyperinsulinemia) in the bloodstream. They also found that the glucose infusion reduced the normal increase in glucose production (release of glucose from the liver), and reduced the amount of free fatty acids released in the bloodstream. The heart rate also did not increase as much as is usually seen in McArdle people during exercise. This may suggest that a sugary drink is most useful for very short term exercise, but not very useful for prolonged exercise. This result may suggest that the body of a McArdle person will try to overcome the lack of muscle glycogen phosphorylase by increasing the activity of a different protein. When there are excess levels of glucose in the body, for example when digestion of meal results in the release of lots of glucose, it is converted into glycogen so that it can be stored until needed. Each isoform is expressed predominantly in the respective tissue; brain, muscle or liver (Newgard et al. The muscle and brain isoforms have greater similarity to each other than to the liver isoform (Hudson et al. The human brain isoform is slightly longer, so that it is 862 amino acids long, compared to 846 for the human liver isoform and 841 for the human muscle isoform. There are control regions located next to each gene to control the location within the body where each isoform is produced. All three isoforms; brain, muscle and liver glycogen phosphorylase break down glycogen into glucose-1-phosphate. In the skeletal muscle of McArdle people, there is no (or very little) muscle glycogen phosphorylase, leading to McArdle disease. Brain glycogen phosphorylase and liver glycogen phosphorylase have not been found in adult skeletal muscle, as shown by the lack of a positive phosphorylase stain in a muscle biopsy from a McArdle person (section 2. Walker (2006) found there to be a gradual decrease of the brain isoform and a concurrent gradual increase of muscle isoform over time in the sheep foetal muscle and sheep neonatal (newly born) skeletal muscle. By 15 days after birth, there was only a trace of the brain isoform in the sheep muscle. However, after muscle damage has occurred, muscle cells divide to produce new cells to replace the damaged cells. Immature muscle cells produce other forms of glycogen phosphorylase which are not the muscle isoform. At present, it is not clear if this is just the brain isoform, just the liver isoform, or both. It should also be noted that much of this information is not based upon humans and is instead based on studies of other mammals such as rat, rabbit, and sheep. To summarise published information, it seems that two general statements could be made about the isoforms of glycogen phosphorylase: Brain and liver glycogen phosphorylase are often found in the same locations; smooth muscle such as bladder, and intestine. My opinions of the expression of different isoforms in the body of a McArdle person are given in Table 6. Part of the body of a Comments in relation to McArdle disease McArdle person Brain Glycogen phosphorylase in the brain of a person unaffected by McArdle disease is approximately 50% brain glycogen phosphorylase and 50% muscle glycogen phosphorylase. It has been suggested that it may have a small effect upon the functioning of the brain but further studies are needed to prove this (see section 10. Skin I believe that skin cells express either brain or liver glycogen phosphorylase (or both). They are unaffected by the absence of muscle glycogen phosphorylase in McArdle disease. Heart Glycogen phosphorylase in the heart of a person unaffected by McArdle disease is approximately 50% brain glycogen phosphorylase and 50% muscle glycogen phosphorylase. This does not appear to have any effect upon the functioning of the heart (see section 13. Lungs these are composed of smooth muscle and express both brain and liver glycogen phosphorylase. Digestive system: these are composed of smooth muscle and express either brain or liver Intestine, digestive tract, glycogen phosphorylase (or both). Muscle glycogen phosphorylase has bladder, liver, kidney been found in the kidneys of rats unaffected by McArdle disease. These organs do not seem to be affected by the absence of muscle glycogen phosphorylase in McArdle disease. Reproductive system: these are composed of smooth muscle and express either brain or liver uterus, testis, probably glycogen phosphorylase (or both). They are unaffected by the absence of muscle 73 ovaries glycogen phosphorylase in McArdle disease. In a person unaffected by entire body: biceps, McArdle disease they would express muscle glycogen phosphorylase. In triceps, quadriceps, a McArdle person no glycogen phosphorylase is present, leading to calves and many others. Nervous system: spinal these express either brain or muscle glycogen phosphorylase (or both). Based upon limited published information (summarised from information reviewed by Wright, 2009) and my opinion. Changing the balance between the amount of protein, carbohydrate, and fat in the diet is a cheap and easy approach to try to improve the amount of energy available to the muscles.
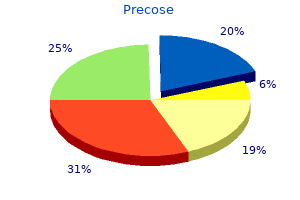
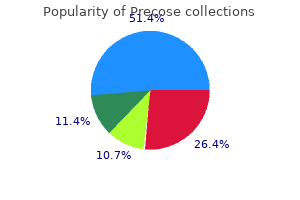
For those in college keck diabetes prevention initiative buy generic precose on line, 2014 data indicate that 6% of college students smoke marijuana daily blood sugar highs and lows discount precose express, while only 2% smoked daily in 1994 diabetic arthropathy generic precose 25 mg visa. For noncollege students of the same age diabetes in dogs client handout buy precose no prescription, the daily percentage is twice as high (approximately 12%). Additionally, according to a recent survey by the National Institute of Drug Abuse (2018), daily cigarette smoking is lower for those in college in comparison to non-college groups (see Figure 7. Rates of violent death are influenced by substance use which peaks during emerging Source and early adulthood. Drugs impair judgment, reduce inhibitions, and alter mood, all of which can lead to dangerous behavior. Reckless driving, violent altercations, and forced sexual encounters are some examples. Drug and alcohol use increase the risk of sexually transmitted infections because people are more likely to engage in risky sexual behavior when under the influence. This includes having sex with someone who has had multiple partners, having anal sex without the use of a condom, having multiple partners, or having sex with someone whose history is unknown. Lastly, as previously discussed, drugs and alcohol ingested during pregnancy have a teratogenic effect on the developing embryo and fetus. Because gender is considered a social construct, meaning that it does not exist naturally, but is instead a concept that is created by cultural and societal norms, there are cultural variations on how people express their gender identity. For example, in American culture, it is considered feminine to wear a dress or skirt. However, in many Middle Eastern, Asian, and African cultures, dresses or skirts (often referred to as sarongs, robes, or gowns) can be considered masculine. Similarly, the kilt worn by a Scottish male does not make him appear feminine in his culture. For many adults, the drive to adhere to masculine and feminine gender roles, or the societal expectations associated with being male or female, continues throughout life. In American culture, masculine roles have traditionally been associated with strength, aggression, and dominance, while feminine roles have traditionally been associated with passivity, nurturing, and subordination. Men tend to outnumber women in professions such as law enforcement, the military, and politics, while women tend to outnumber men in care-related occupations such as childcare, healthcare, and social work. Adherence to these roles may demonstrate fulfillment of social expectations, however, not necessarily personal preferences (Diamond, 2002). Consequently, many adults are challenging gender labels and roles, and the long-standing gender binary; that is, categorinzing humans as only female and male, has been undermined by current psychological research (Hyde, Bigler, Joel, Tate, & van Anders, 2019). The term gender now encompasses a wide range of possible identities, including cisgender, transgender, agender, genderfluid, genderqueer, gender nonconforming, bigender, pangender, ambigender, non gendered, intergender, and Two-spirit which is a modern umbrella term used by some indigenous North Americans to describe gender-variant individuals in their communities (Carroll, 2016). Gender Minority Discrimination: Gender nonconforming people are much more likely to Figure 7. Transgender individuals of color face additional financial, social, and interpersonal challenges, in comparison to the transgender community as a whole, as a result of structural racism. Black Source transgender people reported the highest level of 257 discrimination among all transgender individuals of color. As members of several intersecting minority groups, transgender people of color, and transgender women of color in particular, are especially vulnerable to employment discrimination, poor health outcomes, harassment, and violence. Consequently, they face even greater obstacles than white transgender individuals and cisgender members of their own race. Results indicated that participants who identified as transgender and gender nonconforming had significantly higher levels of anxiety and depression than those identifying as cisgender. The transgender children discussed in chapter 4 may, when they become an adult, alter their bodies through medical interventions, such as surgery and hormonal therapy, so that their physical being is better aligned with gender identity. However, not all transgender individuals choose to alter their bodies or physically transition. Many will maintain their original anatomy but may present themselves to society as a different gender, often by adopting the dress, hairstyle, mannerisms, or other characteristics typically assigned to a certain gender. It is important to note that people who cross-dress, or wear clothing that is traditionally assigned to the opposite gender, such as transvestites, drag kings, and drag queens, do not necessarily identify as transgender (though some do). Sexuality may be experienced and expressed in a variety of ways, including thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles, and relationships. These may manifest themselves in biological, physical, emotional, social, or spiritual aspects. The biological and physical aspects of sexuality largely concern the human reproductive functions, including the human sexual-response cycle and the basic biological drive that exists in all species. Emotional aspects of sexuality include bonds between individuals that are expressed through profound feelings or physical manifestations of 258 love, trust, and care. Sexuality also impacts, and is impacted by cultural, political, legal, philosophical, moral, ethical, and religious aspects of life. In most mammalian species, sex hormones control the ability to engage in sexual behaviors. However, sex hormones do not directly regulate the ability to copulate in primates (including humans); rather, they are only one influence on the motivation to engage in sexual behaviors. Social factors, such as work and family, also have an impact, as do internal psychological factors like personality and stress. Sex drive may also be affected by hormones, medical conditions, medications, lifestyle stress, pregnancy, and relationship issues. The sexual response cycle is a model that describes the physiological responses that take place during sexual activity. According to Kinsey, Pomeroy, and Martin (1948), the cycle consists of four phases: excitement, plateau, orgasm, and resolution. The excitement phase is the phase in which the intrinsic (inner) motivation to pursue sex arises. The plateau phase is the period of sexual excitement with increased heart rate and circulation that sets the stage for orgasm. Orgasm is the release of tension, and the resolution period is the unaroused state before the cycle begins again. The Brain and Sex: the brain is the structure that translates the nerve impulses from the skin into pleasurable sensations. The brain regulates the release of hormones, which are believed to be the physiological origin of sexual desire. The cerebral cortex, which is the outer layer of the brain that allows for thinking and reasoning, is believed to be the origin of sexual thoughts and fantasies. Beneath the cortex is the limbic system, which consists of the amygdala, hippocampus, cingulate gyrus, and septal area. These structures are where emotions and feelings are believed to originate, and they are important for sexual behavior. This is the small area at the base of the brain consisting of several groups of nerve-cell bodies that receives input from the limbic system. Studies with lab animals have shown that destruction of certain areas of the hypothalamus causes complete elimination of sexual behavior. One of the reasons for the importance of the hypothalamus is that it controls the pituitary gland, which secretes hormones that control the other glands of the body. Oxytocin, also known as the hormone of love, is released during sexual intercourse when an orgasm is achieved. Oxytocin is also released in females when they give birth or are breast feeding; it is believed that oxytocin is involved with maintaining close relationships. In males, testosterone appears to be a major contributing factor to sexual motivation. Vasopressin is involved in the male arousal phase, and the increase of vasopressin during erectile response may be directly associated with increased motivation to engage in sexual behavior. The relationship between hormones and female sexual motivation is not as well understood, largely due to the overemphasis on male sexuality in Western research. Estrogen and progesterone typically regulate motivation to engage in sexual behavior for females, with estrogen increasing motivation and progesterone decreasing it. Research suggests that testosterone, oxytocin, and vasopressin are also implicated in female sexual motivation in similar ways as they are in males, but more research is needed to understand these relationships. Sexual Responsiveness Peak: Men and women tend to reach their peak of sexual responsiveness at different ages. For men, sexual responsiveness tends to peak in the late teens and early twenties. Sexual arousal can easily occur in response to physical stimulation or fantasizing.
Order genuine precose line. Reduced 20 kgs Dr Dixit Diet plan weight loss story and Giveaway | How much weight loss Dixit Diet.
Japanese knotweed (Hu Zhang). Precose.
- How does Hu Zhang work?
- Are there safety concerns?
- Constipation, menstrual problems, hot flashes, heart disease, high cholesterol, cancer, skin burns, liver disease, gout, and gallstones.
- Are there any interactions with medications?
- Dosing considerations for Hu Zhang.
- What is Hu Zhang?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97057
Approximately 95% of burns are acci dental; 2% are related to abuse diabetes 1 buy precose 25mg overnight delivery, and 1% are self-inflicted diabetes symptoms passing out discount 50mg precose mastercard. Almost all burns are preventable diabetic diet 6 small meals a day menu purchase precose once a day, and simple measures such as installation of smoke detectors have been highly effective diabetes prevention study order precose 50mg visa. The new england journal of medicine Immediate Management However, most patients with burns do not re quire intubation, because their burns are rela Initial management follows the same principles tively small. The thresh the primary airway concern is upper-airway old for intubation should be low for any patient obstruction, and the key decision is whether to with deep burns occupying more than 30 to 40% place an endotracheal tube. Smaller burns may be massive burns, the airway can swell to the point managed without an endotracheal tube, and since of total obstruction, and early endotracheal intu it takes several hours for maximal swelling to bation is required before the airway is lost. Problem Comments* Airway Is intubation required to prevent Indicators of a requirement for intubation (if in doubt, perform endotracheal intubation): airway obstruction Management of Burns the burn center, where the decision about intu the airways patent)11; for details, see Table S1 in bation can be made. In a common sce Lung damage after smoke-inhalation injury is nario, a patient receiving supplemental oxygen is much more severe when combined with a major burned while smoking a cigarette. Another cause (from propane or butane) are not usually ex of hypoxemia is carbon monoxide; elevated posed to smoke and generally do not have smoke blood levels of carbon monoxide should be con inhalation injury. The pathophysiology of smoke sidered in patients with prolonged smoke expo inhalation injury involves smoke particles that sure. The affinity of carbon monoxide for hemo settle on bronchiolar mucosa, leading to epithe globin is 200 to 250 times the affinity of oxygen lial-cell death, sloughing, small-airway obstruc for hemoglobin; therefore, in the presence of tion, atelectasis, and an increased risk of pneu carbon monoxide, oxygen delivery is substan monia. Measurements of arterial blood9 similar to treatment of the acute respiratory gases and pulse oximeter readings are of no distress syndrome. Measurement Circulation of carboxyhemoglobin is the only accurate test Patients with extensive burns require larger re of carbon monoxide levels, and if levels of car suscitation volumes than patients with any other boxyhemoglobin are higher than 30 to 40%, the type of insult. Because initial resuscitation rates patient has had severe exposure to carbon mon are so high, several formulas have been devel oxide. Treatment consists of the administration oped, which are based on the total body-surface of 100% oxygen. The Rule of Nines estimates of carbon monoxide from hemoglobin decreases that each arm accounts for 9% of total body from 3 or 4 hours to less than 1 hour in the surface area, as does the head, whereas the an presence of 100% oxygen. Hyperbaric oxygen terior trunk and the posterior trunk each ac further reduces the half-life but is rarely admin count for 18%, as does each leg. This rule is istered in patients with massive burns, since it fairly inaccurate, since most people do not have makes management of other burn-related issues the classic body of Atlas (in Greek mythology), difficult. The abdominal burns, compartment syndromes may most important point is that the chart should be develop that require escharotomies (incisions used to estimate only the initial fluid rate. The acute the best-known formula, the Parkland for respiratory distress syndrome occasionally devel mula, estimates the rate of fluid resuscitation ops in a patient with burns. It should be treated for the first 24 hours as 4 ml per kilogram of with the use of low tidal volumes (about 6 ml per body weight per percent of total body-surface area kilogram of predicted body weight, with positive that is burned, with half the volume of fluids end-expiratory pressure levels adequate to keep delivered in the first 8 hours. The new england journal of medicine alternative modified Brooke formula, one may needs,23 but there are questions about whether it consider dropping that value to 2 ml per kilo works primarily as a diuretic. After the initial rate of fluid resus A hospital stay for a patient with massive burns citation has been determined, fluids should be is usually long because weeks to months are adjusted on the basis of urine output (with a required to close the wounds. Half that inevitable bouts of sepsis and multiple organ volume (16,000 ml) should be given in the first dysfunction (Table S2 in the Supplementary Ap 8 hours. The fluid rate should be adjusted on the basis of a target urine output of Addressing the Hypermetabolic Response 50 ml per hour. Patients with deep burns, those A profound hypermetabolic and catabolic re with smoke inhalation and associated injuries, sponse develops in patients with burns covering patients for whom resuscitation is delayed, small more than 20% of total body-surface area, lead children, and patients with alcohol intoxication ing to muscle wasting and, if untreated, death require proportionately more fluid. Minimizing pain and dis hemoglobin values), but they often result in an tress also reduces metabolic demand, but elimi overestimate of fluid requirements. Likewise, minimizing the current problem is that clinicians tend to infection and sepsis reduces metabolic demand provide too much fluid, leading to what has but is very difficult to achieve. Calorie requirements can be calculated with High-dose vitamin C (66 mg per kilogram per the use of various formulas for resting energy hour) has also been reported to reduce fluid expenditure. Because of these problem is interruption of feedings, but most issues, patients with burns are usually excluded centers try to make up for deficits by ignoring all from major sepsis trials. Insulin, insulin-like growth factor 1, and growth hormone have all been shown to have a 1,26,29,31 Burn Wound Care benefit but are rarely used. Oxandrolone is a testosterone analogue without masculinizing the care of burn wounds is based on the depth effects that, at a dose of 10 mg twice a day, im of injury (Fig. Skin is divided into two com proves muscle mass and outcomes in patients ponents: the epidermis and the dermis. Mixed in with the Sepsis in Patients with Burns basal-cell layer are melanocytes with branched Sepsis is a major risk after any large burn be extensions, similar to dendrites, that reach 30 to cause the primary barrier to microbial invasion, 40 keratinocytes and that deliver melanosomes the skin, is lost. Sepsis can develop any time that are phagocytized by the keratinocytes and after resuscitation, and the risk persists as long placed as a protective layer above the nucleus. Unfortunately, anti the dermis does not function as a barrier but biotics are ineffective in preventing infection. The dermis also contains skin adnexa with burns than in most other patient popula such as hair follicles, oil glands, and sweat tions. In ad sure to microbial products combined with the dition, there is a very rich plexus of nerves and hypermetabolic response; all patients with burns vessels coursing through the dermis. The subcu have persistently elevated temperature, tachycar taneous tissue, which is primarily fat, provides dia, and variable white-cell counts. Minimal treatment (analgesia and ventilators, and urinary catheters for prolonged moisturizer) or no treatment is required, and heal periods increases the risk of iatrogenic infections. Since the dermal plexus of monitored for signs of sepsis that are unique to vessels and nerves is intact, the wound will burn injuries, such as dropping platelet counts, blanch with pressure and the pain will be severe. The new england journal of medicine Hair follicle Burn type Epidermis First-degree Basal cells Dermis Second-degree (partial thickness) Arrector pili muscle Oil gland Third-degree Subcutaneous (full thickness) tissue Fascia Fourth-degree Muscle Nerve Arteriole Venule Figure 1. The bottom layer, called the basal-cell layer, has the potential for proliferation and migration after injury. If uninjured, the basal-cell layer differentiates into multiple layers that contain keratin and eventually undergo apoptosis. The dermis is composed mainly of extracellular matrix, which imparts strength to the skin, and contains numerous skin adnexa (hair follicles, oil glands, and sweat glands) that are needed for dermal regeneration. A vascular plexus provides the blood supply, and nerves provide sensation to the skin. A second-degree burn heals through reepitheli wound edge is only 1 to 2 cm, but in superficial alization (Fig. At the wound edge, the basal wounds, the keratinocytes in the remnant hair cells start migrating across the viable wound follicles and other skin adnexa migrate onto the bed. If adnexa tact inhibition, release of local growth factors are close together, such as in the scalp, reepithe (epidermal growth factor, transforming growth lialization is much faster (within 4 to 5 days) factor, and keratinocyte growth factors 1 and 2), than if the adnexa are less densely packed. Keratinocytes patients tend to have fewer hair follicles than in a moist environment can migrate faster than younger patients, so reepithelialization can be those in a wound that becomes dry and develops impaired. The limit of migration from the tients, so the consequences of the burn can be 2354 n engl j med 380;24 nejm. Given enough fewer skin adnexa remain; thus, deeper burns time, contraction can close any wound but leads require more time to heal. Fourth-degree Any wound that requires more than 2 to 3 weeks burns extend into muscle, bone, or tendon and to reepithelialize has a high chance of becoming need to be treated in burn centers, since they a hypertrophic scar. Loose skin and blisters should be de apply skin grafts harvested from another site. Thick blisters on ness of skin), but the donor site must be sutured the palms and soles of the feet may be left intact closed, which limits the size of the graft. The donor site must should be discontinued within a week, since reepithelialize within 2 to 3 weeks in order to they will invariably cause a rash. For small or studies have shown that silver sulfadiazine im medium-size grafts, sheet grafts have the best pairs reepithelialization, so it should be avoided cosmetic outcome (Fig. They are applied after the wound has the meshed pattern obtained with either device been cleaned and, as an alternative to daily will persist for the life of the patient.
Visceral: Pertaining to one of the organs found in the skull diabetic diet chart pdf buy genuine precose, chest diabetes symptoms before diagnosis purchase 50mg precose, abdomen or pelvis (brain diabetic amyotrophy buy generic precose online, lung diabetes facts 2015 order precose with a mastercard, liver, etc. Weakness of the hands may result in difficulty grasping objects; weakness of the legs may result in difficulty walking; weakness of certain muscles in the pharynx may cause difficulty swallowing. Introduction: Neural tube defects are the most common congenital Corresponding author: conditions of the nervous system particularly in the African countries alkarsani@yahoo. Myelomeningocele is the most common form of spina bi fda cystica and is associated with lifelong mortalities and morbidities specially when associated with hydrocephalus. Material and methods: Retrospective review of cases which have been operated at the National Center for Neurological Sciences at Shaab hospital during the period from September 2010 to September 2012. The data obtained from a computerized data record system in the center and the patients clinically assessed by the author when they came for follow up in the refer clinic. Result: In the last two years the center has received 137 cases hav ing this condition, 55. The youngest child operated was 4 days old and the oldest was 5473 days which is approximately equivalent to 15 years old. The mean age at presentation was 274 days which is approximately equivalent to 9 months. Tethered cord release can signifcantly improve symptoms in these patients and reduce the long term effect and complications of this condition. Myelomeningocele occurs in approximately 1 in 2900 live births in the United States. Fobe stated the usual site of the defect which is usually single is that myelomeningocele occurs in 0. The extent of the problem Myelomeningocele is the most common type of spina bifda cystic. The late presentation and preop the incidence in the western community is low after erative infection are associated with high mortality controlling programs, in Africa the incidence is not in those patients. The individuals affected with the presentation of the condition in African children myelomeningocele are experiencing great diffculty may be somewhat late, many factors contributed to in achieving normal milestones of development to this like lack of medical and surgical facilities, high adulthood life [5]. Many patients with myelomeningiocele reach adult hood and social continence; self-care may be ex Higher spinal cord lesion, hydrocephalus and com pected in a large number of patients. Nevertheless, plications due to its surgical management had a there are many associated neurological conditions negative infuence on physical, neurological and that have to be faced. Patients with a myelomeningocele born outside the hospital are prone to infectious complication. The In African countries since there are no national ef most common cause of post-operative death was forts to prevent or compact this condition as the infection (65%). Shunt complications remain an important cause of morbidity and mortality in myelomeningocele pa Cerebral cortical malformations and hydrocephalus, tients; particularly shunt infection [17]. For defects larger than cephalus associated with neural tube defects [12, 25 cm(2) more soft tissue for well-vascularized cov 13]. The surgical treatment of hydrocephalus have to the overall post-operative mortality was 8. The situation in the Sudan Since there is increased incidence of shunt compli cations many experts prefer to perform V-P shunt the national center of neurological sciences in Khar placement and myelomeningiocele repair in sepa toum Sudan has great experience in managing this rate sessions while others suggest to do both in one condition since the early seventies of the last cen session as they think that simultaneous insertion of tury, it was and up to the recent days, the only shunt and correction of a myelomeningocele do not center treating this condition in Sudan. The insertion of a ventriculoperitoneal shunt, at the Retrospective review of cases which have been same session with the repair of the myelomeningo operated at the National Center for Neurological cele, does not increase the risks of shunt infection Sciences at Shaab hospital during the period from or shunt malfunction. The data ob tained from a computerized data record system in the center and the patients clinically assessed by the author when they came for follow up in the refer clinic. Skin over the lesion SwellingCharacteristics Frequency Percent With normal skin covering 70 51. Attention to this condition and establishment of preventive and early discovery and interventions programs is highly important. Awareness of the community and medical profes sionals with impact of this problem with a sector of the community should be raised. In our center the placement of ventriculoperitoneal shunt before surgical repair of the defect help to 6 this article is available from: Fetal surgery for myelomeningocele: of dehiscence of the repair the presence of cere Patient selection, perioperative management and outcomes. Tethered cord release can signifcantly improve Implications of surgical treatment. Arq Neuropsiquiatr 1999; 57 symptoms in these patients and reduce the long (1): 44-50. Interrelationships of sex, level of lesion, further neurological damage and deterioration dur and transition outcomes among young adults with ing surgical intervention and may sometimes help myelomeningocele. Neurological abnormalities, major orthopaedic deformities and ambulation analysis in a Sometimes the presence of the defect might lessen myelomeningocele population in Catalonia (Spain). Results of surgical treatment of contribute to delayed presentation and in some myelomeningocele. Sonographic prenatal ous shunting may lead to development of acute diagnosis of central nervous system abnormalities. Maldevelopment of the cerebral cortex in the early but late presentation is encountered from time surgically induced model of myelomeningocele: Implications for to time. Reduced hindbrain herniation after intrauterine myelomeningocele the establishment of spina bifda association join repair: A report of four cases. Hydrocephalus associated with neural tube defects: relations with local, regional and international cor Characteristics, management, and outcome in sub-Saharan Africa. Combined endoscopic third stigma of the condition and reducing the psycho ventriculostomy and choroid plexus cauterization as primary logical and fnancial burden on the families of the treatment of hydrocephalus for infants with myelomeningocele: patients. Long-term results of a prospective intent-to-treat study in 115 East African infants. Anesthetic concerns and perioperative the effort of Sudan government, the ministry of complications in repair of myelomeningocele: A retrospective health and the national center of neurological sci review of 135 cases. Long-term survival of individuals with review their cases and share clinical knowledge. Among54articlesinthisera,atotalof in31articleswere included in the current evaluation. Additional signs and symptoms could include huge posterior fossa, sun set sign, seizures, spasticity, apnea, respiratory failure, delayed milestones, hydrocephalus, and increased intracranial pressure. Even though it is usually treated for related hydrocephalus, the abnormality causes no de tectable clinical syndrome. Prognosishasenhancedmeaningfully from the time of its original report; yet, it is typically dependent on the accompanying abnormalities. Keywords: Dandy-Walker Syndrome, Malformation, Diagnosis, Managements, Children 1. Although in contrast to various, fourth ventricle cystic dilation, and expansion of the physical illnesses in children, such as trauma, spine dis posterior fossa. Hydrocephalus is not an obligatory eases, behavioral disorder, and hydrocephalous, (7-10), the nding. The about the best treatment option for this condition in pedi malformation was then described by Dandy and Walker in atric patients. PubMed and Ovid were searched using the following key words: Dandy-Walker syndrome, posterior fossa, pediatric, 3. The criteria involved studies Regarding the assessment of fetal abnormalities, stud from journals that described Dandy-Walker syndrome pe ies have notied about restrictions caused by diagnosis diatric patients. Although some old primary references in with ultrasound being conicting with diagnosis in post this era had to be used, yet based on the philosophy of natal or postmortem pathologies (18). Signicant training and publishing the possibility for related inherited anomalies and occur in this eld is very limited. Among 54 articles in this era, a rence of developmental and cognitive discrepancies (18, total of in 31 articles were included in the current evalua 19). Chromosomal abnormalities Cerebellar growth starts in the 9th week of pregnancy occurinapproximately50% of patients. In famil wards, the vermis is created when the hemispheres join to ial forms, inheritance patterns might be X-linked or auto gether.